

Deep Vein Thrombosis (DVT) : Note For Doctors
") |
| Deep Vein Thrombosis (DVT) |
- Deep Vein Thrombosis (DVT): The formation of a thrombus (blood clot) within the deep veins, most commonly in the lower extremities. If untreated, it can lead to severe complications such as pulmonary embolism (PE).
Pathophysiology:
- Virchow’s Triad: Three key factors contributing to thrombogenesis:
- Stasis of blood flow (e.g., immobility, prolonged sitting, heart failure)
- Endothelial injury (e.g., trauma, surgery, catheter insertion)
- Hypercoagulability (e.g., genetic disorders like Factor V Leiden, malignancy, pregnancy)
- Clot formation begins when platelets adhere to the endothelial surface, followed by fibrin deposition and aggregation of blood cells. The clot can extend, causing venous obstruction.
 |
| virchows triad |
Etiology and Risk Factors:
- Primary Risk Factors:
- Prolonged immobility (post-surgery, prolonged bed rest, long-duration travel)
- Surgical procedures (especially orthopedic surgeries: hip, knee)
- Trauma (fractures, surgery, etc.)
- Malignancy (increased clotting tendency due to tumor-derived procoagulants)
- Pregnancy and postpartum (due to increased estrogen levels and venous stasis)
- Oral contraceptives and hormone replacement therapy (estrogen increases clotting risk)
- Genetic thrombophilia (e.g., Factor V Leiden mutation, Prothrombin gene mutation)
- Secondary Risk Factors:
- Age > 60 years
- Obesity
- Family history of DVT or PE
- Smoking
- Chronic conditions like heart failure, varicose veins, and inflammatory bowel disease.
Clinical Presentation:
- Common Symptoms:
- Unilateral leg swelling: Most common clinical feature, often with a sense of heaviness.
- Pain: Deep, aching pain in the affected leg, aggravated by standing or walking.
- Erythema: Redness and warmth over the affected area.
- Palpable cord: The thrombus may feel like a firm, rope-like structure along the affected vein.
- Classic Signs:
- Homan’s sign: Pain on dorsiflexion of the foot (not highly sensitive or specific).
- Positive Homans or Lowenberg test: Pain with calf compression, though less commonly used in modern clinical practice.

Complications:
- Pulmonary Embolism (PE): The most serious complication. Clots from DVT may dislodge and travel to the pulmonary circulation, causing a blockage.
- Post-thrombotic Syndrome (PTS): Chronic condition resulting from long-term venous hypertension, causing pain, swelling, and skin changes.
- Chronic Venous Insufficiency: Due to damage to venous valves, leading to chronic swelling and skin changes.

Diagnosis:
-
Clinical Assessment:
- Clinical probability can be assessed using the Wells score (for DVT and PE), which factors in risk factors and clinical presentation.
-
Ultrasound (Doppler):
- The gold standard for diagnosing DVT. High-frequency ultrasound assesses for the presence of a thrombus, venous compression, and blood flow.

- The gold standard for diagnosing DVT. High-frequency ultrasound assesses for the presence of a thrombus, venous compression, and blood flow.
-
D-dimer:
- Elevated D-dimer levels indicate fibrin degradation products, suggesting clot formation. However, it lacks specificity, and can be raised in other conditions (e.g., infection, cancer).
- Sensitivity >95%, but specificity is low, especially in low-risk patients.
-
CT Venography/Magnetic Resonance Venography (MRV):
- Used in selected cases when ultrasound is inconclusive or inaccessible.
-
Contrast Venography:
- The gold standard historically but is less commonly used today due to its invasiveness and the rise of ultrasound.
Management:
-
Anticoagulation Therapy:
- Initial Treatment:
- Low molecular weight heparin (LMWH) (e.g., enoxaparin) or unfractionated heparin (UH) for immediate anticoagulation.
- Direct oral anticoagulants (DOACs) (e.g., rivaroxaban, apixaban) as an alternative to LMWH.
- Long-term Management:
- Warfarin (Coumadin), INR monitored (goal INR 2.0-3.0), or continued use of DOACs for 3-6 months based on risk factors and the nature of the clot.
- Initial Treatment:
-
Thrombolysis:
- Recombinant tissue plasminogen activator (rt-PA) or urokinase for large, symptomatic clots or in cases with life-threatening PE. Reserved for severe cases.
-
Thrombectomy or Catheter-directed Thrombolysis:
- Surgical intervention or catheter-based removal may be considered in patients with massive DVT or failure of anticoagulation therapy.
-
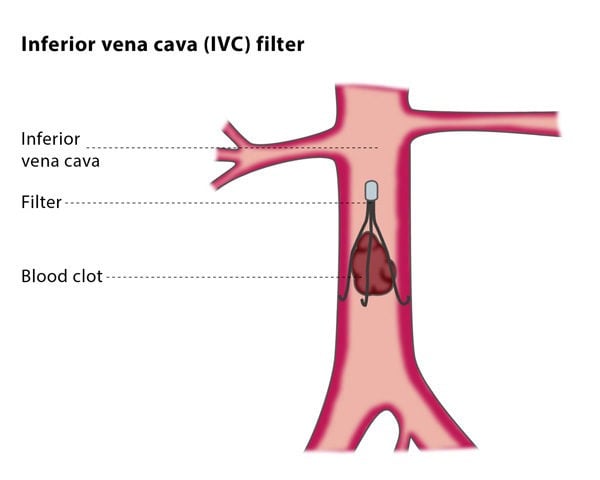
Inferior Vena Cava (IVC) Filter:
- Used in patients with contraindications to anticoagulation (e.g., active bleeding) or recurrent PE despite anticoagulation therapy.
-

Compression Stockings:
- Used to reduce swelling, prevent post-thrombotic syndrome, and improve venous return in chronic cases.
Prevention:
- Prophylaxis:
- Early mobilization and exercises for hospitalized patients.
- Low-dose heparin or LMWH for high-risk surgical patients.
- Intermittent pneumatic compression devices for critically ill patients.
- Compression stockings for those at risk, especially post-operatively.
Follow-up and Monitoring:
- Regular monitoring of anticoagulation levels, especially for warfarin (INR monitoring), and for signs of bleeding complications.
- For patients on DOACs, renal function should be monitored periodically.
Tip of the day

