Comparison of the Subjective vs. Objective Tinnitus for ENT

Definitions of Tinnitus Types
-
Subjective Tinnitus (S-Tinnitus):
A perception of sound (e.g., ringing, buzzing, hissing) heard only by the patient, with no actual external or internal sound source detectable by others. It is the most common form of tinnitus. -
Objective Tinnitus (O-Tinnitus):
A rare form of tinnitus where a real sound is generated within the body (e.g., by vascular or muscular activity) and can sometimes be heard by an examiner using a stethoscope.
Comparison Table: Subjective vs. Objective Tinnitus
| Feature | Subjective Tinnitus | Objective Tinnitus |
|---|---|---|
| Perception | Heard only by the patient | Can be heard by examiner (with tools) |
| Cause | Often neurological or auditory | Usually mechanical or vascular |
| Common Examples | Noise-induced hearing loss, ototoxic drugs | Vascular bruits, palatal myoclonus |
| Prevalence | Very common (>95% of cases) | Very rare (<5% of cases) |
| Audibility to Others | Not audible to others | Audible to others (e.g., with stethoscope) |
| Sound Characteristics | Ringing, buzzing, hissing | Pulsatile or clicking |
| Associated Disorders | Cochlear damage, Meniere’s disease | AV malformations, muscle spasms |
| Diagnostic Approach | Audiometry, MRI, ENT exam | Stethoscope exam, Doppler, imaging |
| Treatment Focus | Symptom management, sound therapy | Treat underlying physical cause |
Let me know if you’d like this in a downloadable format or visual chart.
Objective tinnitus is a rare form of tinnitus where the sound can actually be heard by an examiner, often through a stethoscope placed near the ear. It is usually caused by internal bodily sounds, and often has a physical/mechanical source. Here’s a list of common causes of objective tinnitus:
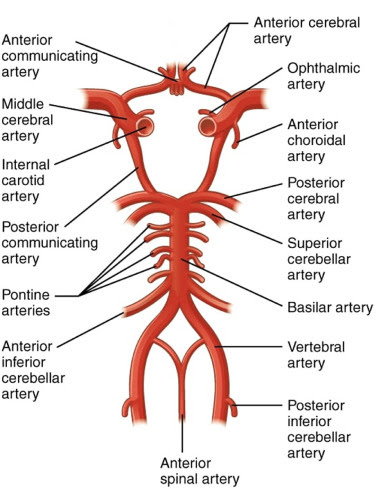
Vascular Causes (Pulsatile Tinnitus)
-
Arteriovenous malformations (AVMs)
-
Carotid artery stenosis or dissection
-
Glomus tumors (paragangliomas)
-
Dural arteriovenous fistulas
-
Aberrant carotid artery
-
Persistent stapedial artery
-
Increased intracranial pressure (e.g., idiopathic intracranial hypertension)
-
Venous hums (especially in high-flow states like anemia or pregnancy)
Muscular Causes (Myoclonic Tinnitus)
-
Tensor tympani muscle spasms
-
Stapedius muscle spasms
-
Palatal myoclonus (rhythmic contractions of the soft palate)
-
Middle ear myoclonus (can involve both tensor tympani and stapedius)
Patulous Eustachian Tube
-
Abnormally open Eustachian tube – allows internal sounds (like breathing or voice) to be heard more clearly.
Other Causes
-
Vascular tumors near the ear (e.g., hemangiomas)
-
High cardiac output states (e.g., hyperthyroidism, anemia)
Would you like a diagram showing where these conditions occur in the head and ear?