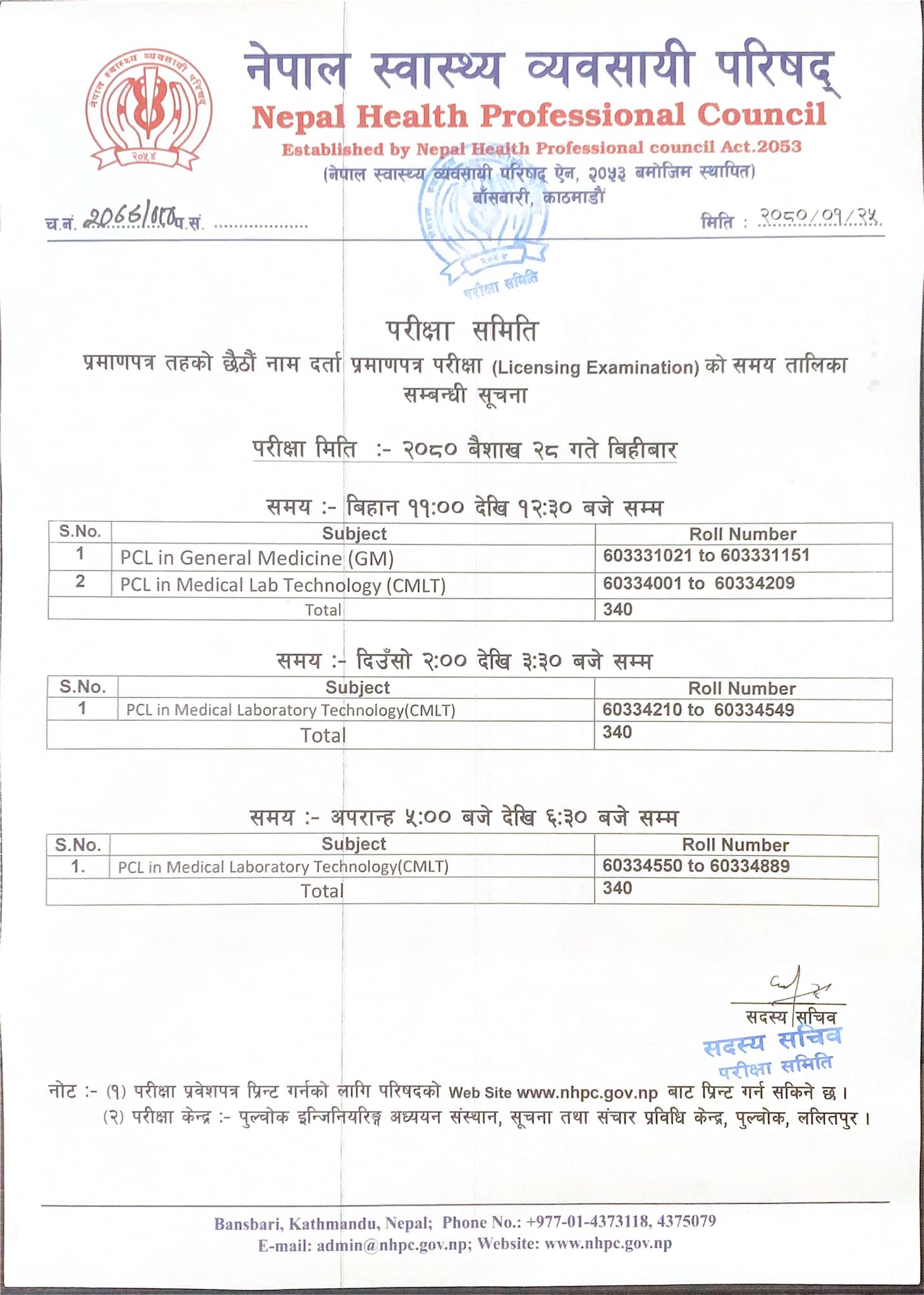
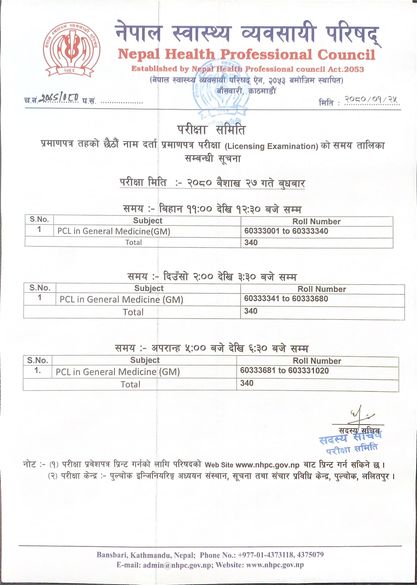
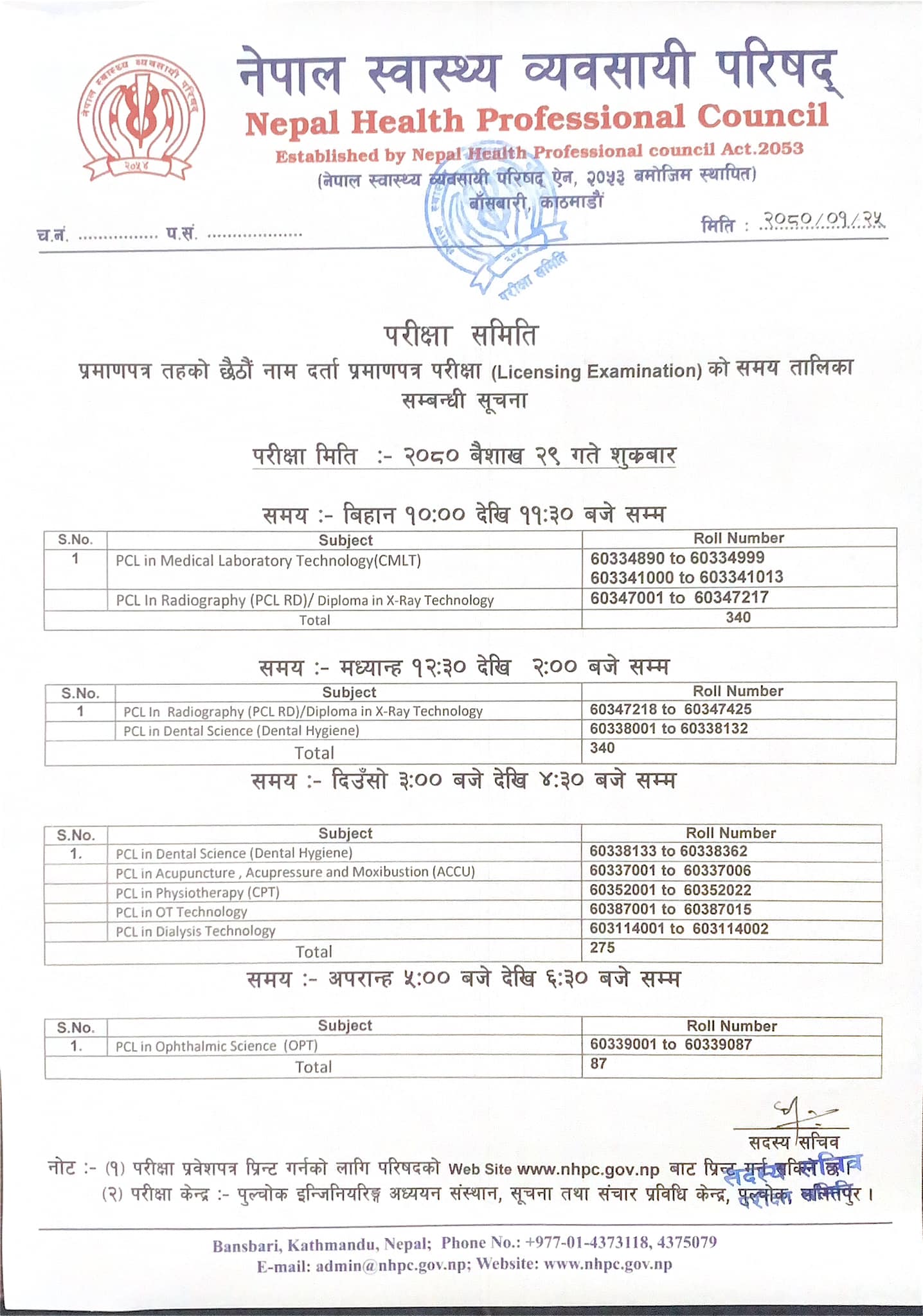
seventh 7th licensing examination full notice from NHPC
How to fill up NHPC licensing examination form:
You must have an active gmail account to fill up form if you appeared in 1st to 5th examination. If you have already used that gmail account for taking exam previously create new one here .
Unveiling the Intricacies: The Anatomy and Physiology of Ventilator Machines
Introduction:
Understanding the anatomy and physiology of ventilator machines is crucial in comprehending the life-saving mechanics behind these essential medical devices. This search engine optimized article delves into the intricate details of ventilator machines, exploring their anatomy and physiology to provide a comprehensive understanding of their crucial role in patient care.
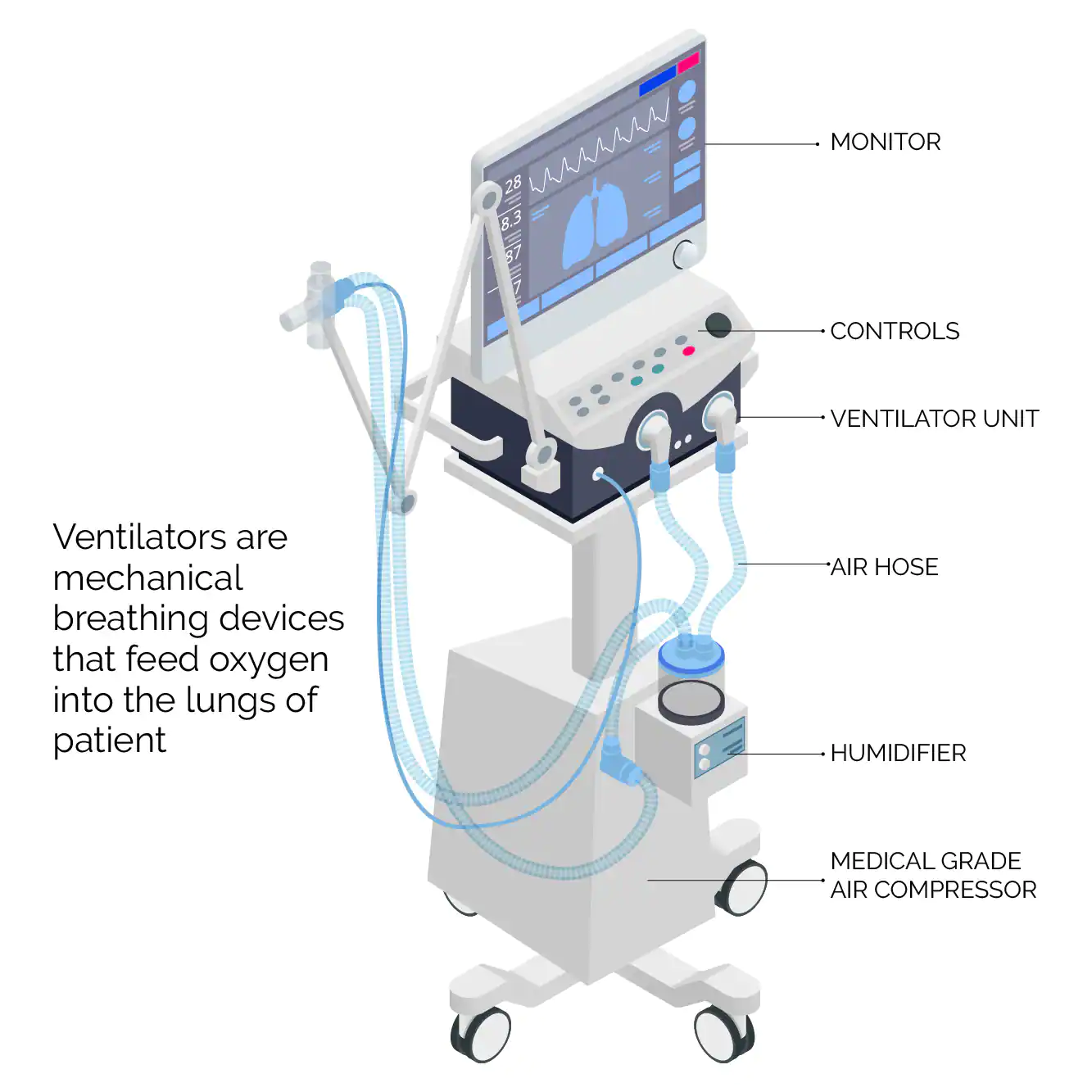
A ventilator machine
1. The Basics: What is a Ventilator Machine?
A ventilator machine, also known as a mechanical ventilator, is a sophisticated medical device used to provide respiratory support to patients in critical care situations. It delivers oxygen to the lungs and removes carbon dioxide, assisting patients in breathing when they are unable to do so independently.
2. Key Components of a Ventilator Machine:
Ventilator machines consist of several essential components that work together to facilitate effective respiratory support. These components include:
– Control Panel:
The control panel allows healthcare professionals to adjust various settings, such as the volume and rate of airflow, to meet the patient’s specific needs.
– Breath Delivery System:
This system comprises an inspiratory limb, expiratory limb, and patient interface. It controls the flow of gases into and out of the patient’s lungs, ensuring proper ventilation.
– Sensors and Monitors:
Ventilators are equipped with sensors and monitors to measure various parameters, such as air pressure, oxygen levels, and patient-ventilator synchrony. These measurements aid in monitoring and adjusting the ventilation process.
3. Physiology of Ventilation:
Ventilator machines function based on the principles of respiratory physiology. The primary modes of ventilation include:
– Pressure-controlled ventilation:
This mode delivers breaths at a set pressure level, ensuring consistent airflow and oxygenation.
– Volume-controlled ventilation:
In this mode, the ventilator delivers breaths at a predetermined volume, maintaining a specific tidal volume for optimal gas exchange.
– Assisted ventilation:
Some ventilators are designed to synchronize with the patient’s spontaneous breaths, providing support when needed and allowing for a more natural breathing pattern.
4. Advanced Features and Modes:
Modern ventilator machines are equipped with advanced features and modes to cater to diverse patient requirements. These may include:
– Positive End-Expiratory Pressure (PEEP):
PEEP helps keep the airways open during exhalation, preventing alveolar collapse and improving oxygenation.
– Pressure Support:
This mode assists the patient’s spontaneous breaths by providing additional pressure support during inhalation.
– Non-invasive Ventilation:
Some ventilators offer non-invasive ventilation options, such as mask-based interfaces, for patients who do not require intubation.
Conclusion:
Understanding the anatomy and physiology of ventilator machines is vital for CEOs in the healthcare industry. This search engine optimized article has provided a comprehensive overview of the essential components and functions of ventilator machines, shedding light on their critical role in providing life-saving respiratory support. By grasping the mechanics behind these devices, CEOs can make informed decisions and contribute to the advancement of patient care.
NHPC license examination 2080 notice detailed with how to print the admit card
Nepal Health Professional Council (NHPC) is an autonomous body established under the Nepal Health Professional Council Act 2053. The aim of this council is to register all the “Health professionals” other than Medical doctors , Nurses , Pharmacists, and Ayurveda according to their qualification; and bring them into a legal system as to make their services effective with quality and timely in a scientific manner.
The mechanical ventilation is basically a replaement of assistance to the spontaneous ventilation/ breathing.
The concept of mechanical ventilation was first introduced by a scientist “Andreas Vesalius in 1555“
He said that : “an opening must be attempted in the trunk of the trachea, into which a tube of reed
or cane should be put; you will then blow into this, so that the lung may rise again . . .
and the heart becomes strong”
This was the fundamental of development of mechanical ventilation and intubation but it took 400 years to apply this and actually use it in medical field.
Now a days mechanical ventilation has been the very vital part of medical sciece and has been used for many purposed in daily basis for saving millions of the lives worldwide.
Mecahnical ventilation and mechanicala ventilators have been used to save lives in emergency situations as well as in elective and emergency surgeries. They are the majr part of modern day ICU care.
The first use of assisted ventilation (nt mechanical ventilations) was done in Europe during Polio outbreak (Read more about polio here).
Back then even human were used to a rtificailly ventilate the lung of sick people making them the human ventilators, and they even worked upto 8 hours a day and the medical schools were shut down for same purpose.
Later a company named “Ëmerson company” made a prototype positive pressure ventilator which was used in the Massachusetts General Hospital and it became instant succcess and started the era of Modern day intennsive care medicine.
What is Mechanical Ventilation? What happens when youre on a ventilator?
The basic concept of mechanical ventilation or positive pressure ventilation is to create a positive pressure the moves air/oxygen into the lungs. DUring breathing the pressure in our alveoli keeps on changing and during inspiration it becomes subatmospheric which drags air into the lungs and aveoli.
But if a person is not able to breathe by themselves in that condition positive pressure more than that of alveoli and lungs needs to be created by using artificial means and air or oxygen is pushed into the lungs.
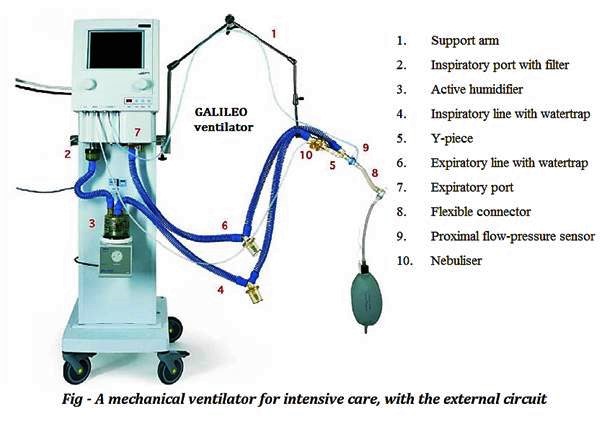
A ventilator machine labelled different parts
Mechanical Ventilation Definition
By undertanding above concept, mechanical ventilation can be difined as a process in which the lungs of a person who is not able to breath by oneself are inflated using external force, person or machine in order to push air into them and pull it back, in order to complete gaseous exchange, or for purpose of delivering medicine (in case of anesthesia or other critical care).
Understanding Mechanical Ventilation Settings
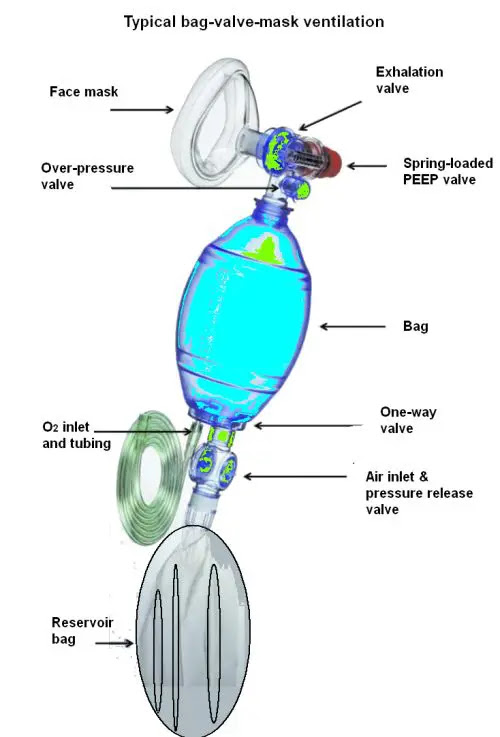
a bag-valve-mask
In general there are two methods of positive pressure ventilation:
Volume controlled ventilation VC mode:
In this mode the initially the volume of air that is needed to be pushed into the ungs is selectd and ventilator selects the pressure needed to push that much volume into lungs by itself. Depending on that the rate of lung inflation, that if respiratory rate can be kept constant ot adjusted.
Pressure control ventilation PC mode:
In this mode the pressure at which the air/oxygen is pushed into lungs is preselected and duration and rate of lung inflation can be adjusted on the basis of need by the operator or doctor. by this desired tidal volume and sufficient oxygenation can be achieved.
The rate of lung inflation is initially high then is reduced so that presssure is same throughout(constant).
In other classification it can be classified as invasive and noninvasive ventilation:
Invasive ventilation
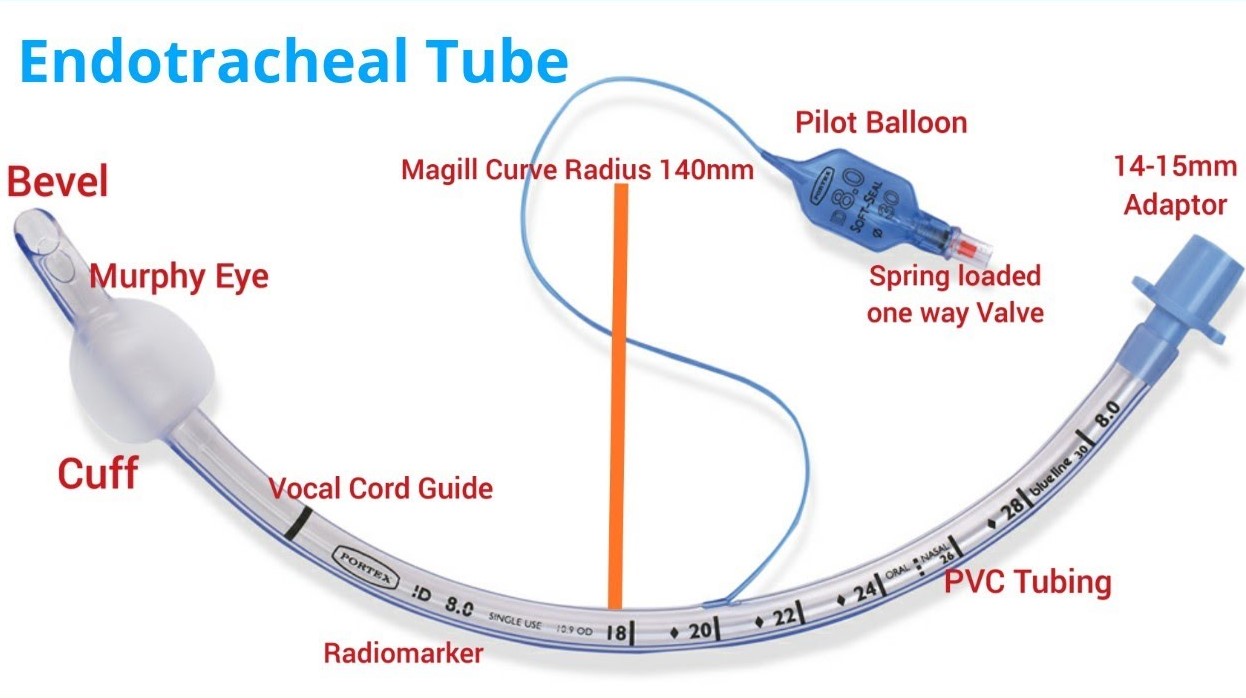
Invasive ventilation means ventilation with intubation in which a person a person has Endotrachea tube (ET Tube) placed in his trachea and through this air is supplied or his lungs are ventilated.
Endotracheal tube
Non-inasive ventilation
Non invasive ventilation consists of CPAP and BiPAP. CPAP standa for continuous positive pressure ventilation and BiPAP mean bilevel positive pressure ventilation.
These both are achieved through a fitting mask kept covering nose and mouth of the patient.
Though these types of ventilation can also be achieved in invasive ventilation as well, unless not necessary a person is not intubated but CPAP / BiPAP mas is used for this purpose.
Volume control Vs Pressure control technique in mechanical ventilation
Invasive Mechanical Ventilation: Benefits and Risks
Indication of mechanical ventilation
Respiratory failure
Hypoxemic respiratory failure : low oxygen saturation (sa02 or sp02)
Hypercarbic respiratory failure: High carbondioxide content in blood (paCO2)
Acute respiratory failure
Ventilatory failure
To reduce cerebral blood flow in case of raise ICP
Prevent aspiration of gastric content or other foreign body
Protect airway in seerely ill patient
In intoxicated, poisoned patients
To delever medicine and artificially breathe in case of general anesthesia
Hemodynamic instability
Heart attack
Head, face and neck surgery
Unstable or risky airway
Cardiac arrest
Encephalopathy
Coma or deterirating GCS
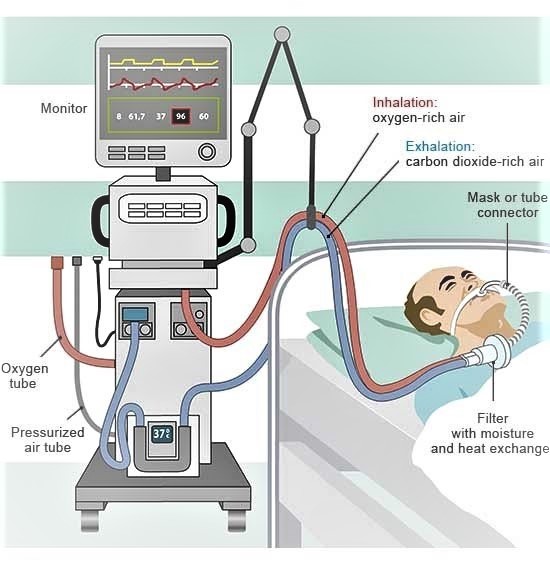
Ventilated patient depiction drawing
Befefits of mechanical ventilation:
Proper and adequate oxygenation
Accurate measurement of pressure and volumes
Decreases work of breathing
Improves gas exhange
Reduces mortality
Low failure rate than noninvasive ventilation
Improves general pulmonary function
Multiple modes available and settings can be changed according to need
Stabilize and protects the airwat from collapse or obstruction
Prevents aspiration
Prevents atelectasis
No airleaks
Risks associated with mechcanical ventilation:
High pressure related lung injury : Barotrauma
Volume trauma
Oxygen toxicity
Ventilator dependence
Infection of airway
Pneumonia, also called VAP : Ventilator associated pneumonia
Mucus plug and lung collapse
Airway trauma, mediastinal perforation
Cuff presure injury to trachea and fistula formation, tracheal necrosis
Hemodynamic collapse
Tube malposition
Electrolyte and aid base imbalance
Mouth, teeth and lip trauma
Infection of sinuses
Muscle weakness and wasting and difficulty breathing after intubation later
Position related complication
Deep venous thrombosis and Pulmonary embolism (PE)
Presure sores, ulcers
Psychaitric problems
Vocal cord injury and difficulty prducing speech
Mechanical Ventilation Systems: Types and Components
Invasive ventilator with modern mamchine
Bag-valve-mask ventilator (manual)
Though bag valve mask can also be connected to endotracheal tube.
ventilator
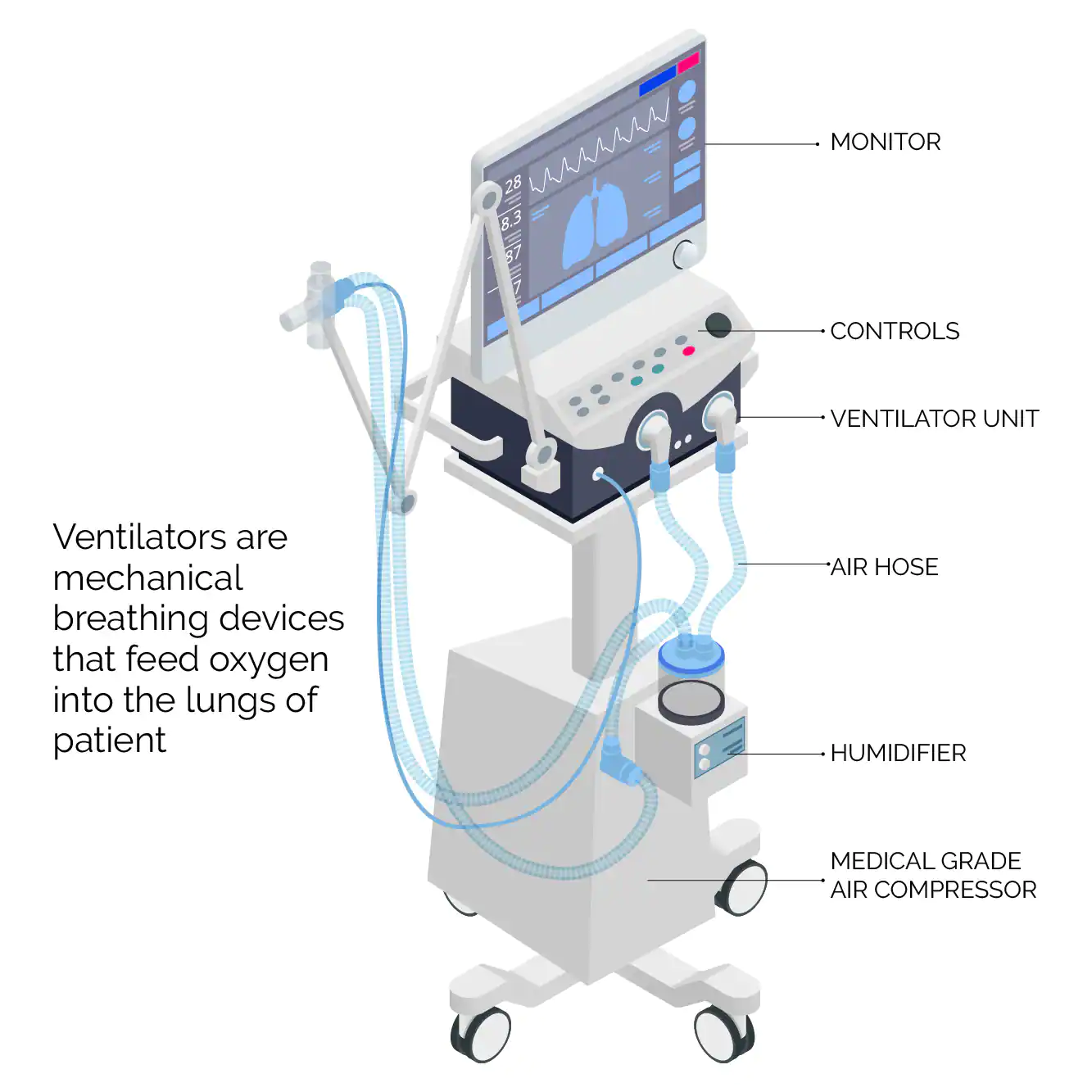
Components of mechanical ventilator:
Connector tube
circuits
t-piece
HME filter
monitor
air and oxygen ports and supply
ventilator machine
power supply
control knobs and butttons
ventilator parts
Instruments needed for mechanical ventilation
Ventilator machine
Connecting tubes for oxygen deivery
Endotracheal ET tube
Syringes
Stethoscope
Direct laryngoscope
Bag-Valve-Mask
Suction machine
Suction tube
Source of oxygen
Fixating tapes/dresings
Medications for anesthesia and muscle relaxation
Monitor for vitals monitering
Trained manpower
Process of putting one into mechanical ventilator or starting mechnical ventilation
The patient is decided for mechanical ventilation on basis of above mentioned criteria
Patient is preoxygenatied
Rapid sequence intubation is done using anesthetic agent and muscle relaxants
Once intubation is done then patient is connected to ventilator machine with appropriate setttings
The settings of the ventilator can be changed as need and patiend is intensively monitored
Regularly check ABG to maintain arterial blood ga and electrolyte in limits
Keep arterial blood pH 7.35-7.45
Reularly check patient efforts, improvements, and treat the condition and cause of patiet’s need of intubation
Follow strict precaution for infection prevention
Prevent other complication
How does a ventilator work
Method of ventilation-Lung Protective ventilatory strategy
Set tidal volume to 6ml/kg
calculate ideal body weight
use VC and set initial tidal volume Vt to 8 ml/kg
set RR to match baseline minute ventilation but not >35 bpm
set PEEP to 5 cm of H2O
reduce Vt by 1 ml/kg every 1-2 hr till its 6ml/kg
adjust PEEP and FiO2 to maintain SpO2 88-95%
Prevent plateau pressure exceedig 30 cm of water
if plateau pressure .30 cm of water and Vt 6 ml/kg decrease vt 1 ml/kg until plateau pressure falls below 30 cm of water or Vt reached minimum of 4ml/kg
use least possible concentreation of oxygent (fraction of inspired oxygen or FiO2) to maintain saturation more than 90%
Adjust PEEP to maintain alveolar potency while preventing overdistention and closure reopening
Ph goal to 7.30 to 7.45
if pH 7.15-7.30 increase RR until ph >7.3, paco2 <25 or RR = 35
if pH <7.15, increase RR=35. if still remains <7.15, increase Vt in 1ml/kg until pH>7.15
if pH>7.45 decrease RR if possible
Read Normal ABG finding of a health person here:
Care during mechanical ventilation:
Sedation and muscle relaxants or paralysis
Analgesia
Intensive monitoring
Chest physiotherapy
Suctioning and secretion clearing
Nutrition
Humidification
Prevention of infection: common site of infections include lungs, urine, oral cavity, skin, and blood
Mobilization
Pressure prevention
Thromboembolic prophylaxis
Skincare
Oralcare
Eye care
Other general care
ventilator in action
Indication for discntinuation mechanical ventilation or indication of extubation
Patients recovery
Weaning
Completion of indication
Death
Technique of weaning:
SIMV wean PS wean T-piece trial
Some terminlogies related to mechanical ventilation:
Respiratory rate RR
Number of breathes (insiration and expiration = one breathe) per minute
Tidal volume Vt
The volume of air inhaled or exhaled in each breath / respiration by the person
Minute ventilation MV
Total volume inhald or exhaled by the person in a minute
FiO2
Fraction of the inhaled oxygen i.e percentage of oxygen in inhaled air
Peak pressure
The maximum pressure during inspiration generated by machine to push air into the lungs.
PEEP
Positive end expiratory pressure. It is the pressure at aveoli at the end of the expiration cycle before beginning of inspiration.
Mechanical ventilation is a medical technique that replaces or assists spontaneous breathing. The concept was first introduced in 1555 by Andreas Vesalius, but it took 400 years to develop mechanical ventilation into a medical practice.
Today, mechanical ventilation and ventilators are widely used for various purposes in medical care, including elective and emergency surgeries and emergency situations. There are two main methods of positive pressure ventilation, volume-controlled and pressure-controlled ventilation, which can be invasive or noninvasive.
Mechanical ventilation has many benefits, such as improving gas exchange, reducing the work of breathing, and improving general pulmonary function, but there are also risks, such as high pressure or lung damage. Overall, mechanical ventilation has been a crucial part of modern-day intensive care medicine and has saved millions of lives worldwide.
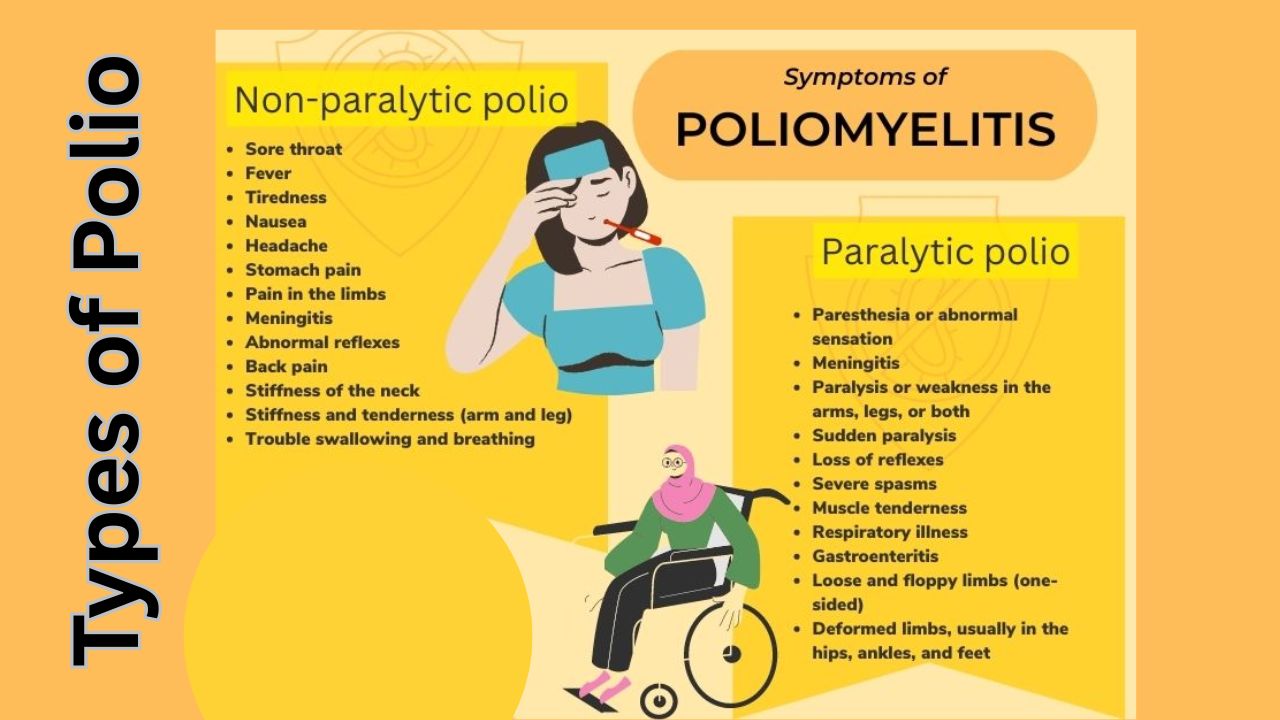
Poliomyelitis, commonly known as polio, is a highly contagious viral disease caused by the poliovirus. It primarily affects the nervous system and can lead to paralysis, permanent disability, or even death in severe cases. Polio mostly affects children under the age of five, but it can also infect unvaccinated adults.
Types of Poliomyelitis
1. Non-paralytic polio: This form causes flu-like symptoms but does not lead to paralysis.
2. Paralytic polio: The most severe form, leading to muscle weakness, loss of reflexes, and paralysis. Paralysis can be permanent.
3. Post-polio syndrome (PPS): This can occur years after recovery, causing muscle weakness, fatigue, and pain.
Transmission
Polio spreads through:
Fecal-oral route: Contaminated food or water.
Person-to-person contact: Through saliva or respiratory droplets.
Prevention
Polio has no cure, but it can be prevented with vaccines:
Oral Polio Vaccine (OPV).
Inactivated Polio Vaccine (IPV).
Global vaccination programs have significantly reduced polio cases, bringing the disease close to eradication.
Causes of Polio
Polio is caused by the poliovirus, a highly infectious virus that belongs to the Picornaviridae family. It primarily spreads through the fecal-oral route, often in areas with poor sanitation, where contaminated food or water can transmit the virus. It can also spread through direct contact with an infected person’s saliva or respiratory droplets. Once inside the body, the virus multiplies in the throat and intestines before entering the bloodstream and, in some cases, attacking the central nervous system. This attack can lead to inflammation and destruction of motor neurons, resulting in paralysis. Poor hygiene, lack of vaccination, and overcrowding increase the risk of transmission.
Symptoms of Polio
Mild cases may show no symptoms. Severe cases can present:
Fever, sore throat, and fatigue.
Muscle stiffness and pain.
Sudden paralysis in severe cases.
How is Polio Diagnosed?
Polio is diagnosed through a combination of clinical evaluation and laboratory tests. A healthcare provider may suspect polio based on symptoms such as acute flaccid paralysis, fever, muscle weakness, and reduced reflexes.
To confirm the diagnosis, laboratory tests are conducted on samples of throat secretions, stool, or cerebrospinal fluid (CSF) to detect the presence of the poliovirus.
Stool samples are the most reliable for isolating the virus. In some cases, molecular techniques like polymerase chain reaction (PCR) are used to identify the virus’s genetic material.
Early and accurate diagnosis is essential for managing the disease and preventing its spread.
Prevention and Treatment of Polio
Polio prevention is primarily achieved through vaccination. The Oral Polio Vaccine (OPV) and the Inactivated Polio Vaccine (IPV) are highly effective in protecting against your disease. OPV is widely used in mass immunization campaigns, particularly in endemic areas, while IPV is administered via injection and is part of routine immunization schedules in many countries. Maintaining good hygiene, proper sanitation, and access to clean drinking water also help reduce the risk of transmission.
Treatment for polio focuses on supportive care, as there is no cure for the disease. This includes managing symptoms, such as using pain relievers, physical therapy to reduce muscle stiffness, and mobility aids like braces or wheelchairs for those with paralysis. In severe cases, mechanical ventilation may be necessary if breathing muscles are affected. Rehabilitation programs can help improve quality of life for individuals recovering from polio or managing post-polio syndrome.
Post-Polio Syndrome: Understanding the Long-Term Effects
The Global Efforts to Eradicate Polio
Global efforts to eradicate polio have been spearheaded by initiatives like the Global Polio Eradication Initiative (GPEI), launched in 1988. This collaborative effort involves organizations such as the World Health Organization (WHO), UNICEF, Rotary International, and the Centers for Disease Control and Prevention (CDC), among others. These programs focus on widespread vaccination campaigns, surveillance to detect and respond to outbreaks, and improving access to clean water and sanitation in high-risk regions. As a result, polio cases have declined by over 99%, with wild poliovirus now endemic in only a few countries, such as Afghanistan and Pakistan. Continued global collaboration and funding are crucial to overcome challenges like vaccine resistance, conflict, and gaps in healthcare systems to achieve a polio-free world.
Polio vaccine
The polio vaccine is a crucial tool in preventing poliomyelitis and achieving global eradication of the disease. There are two primary types of polio vaccines: the Oral Polio Vaccine (OPV) and the Inactivated Polio Vaccine (IPV). OPV is administered orally and contains a weakened form of the virus, which stimulates strong immunity and can also reduce community transmission through shedding of the weakened virus. IPV, given by injection, uses an inactivated (killed) virus to provide individual protection without the risk of vaccine-derived poliovirus.
Both vaccines are safe and effective, with IPV being the preferred choice in countries with robust healthcare systems. Mass immunization campaigns using OPV have been instrumental in significantly reducing global polio cases, while routine immunization programs with IPV help maintain long-term immunity in polio-free regions.
Polio vaccine storage
Proper storage of the polio vaccine is critical to maintaining its effectiveness. Both the Oral Polio Vaccine (OPV) and the Inactivated Polio Vaccine (IPV) are sensitive to temperature changes and must be stored under strict conditions. OPV requires storage at temperatures between -20°C to -25°C, typically in freezers, to preserve the live attenuated virus. IPV, on the other hand, should be stored at temperatures between 2°C to 8°C in a refrigerator.
Vaccines should be kept in insulated containers during transportation to maintain the cold chain and prevent spoilage. Any exposure to higher temperatures or freezing (in the case of IPV) can degrade the vaccine’s potency. Adhering to proper storage protocols ensures the vaccines remain effective, especially in areas with limited infrastructure or during mass immunization campaigns.
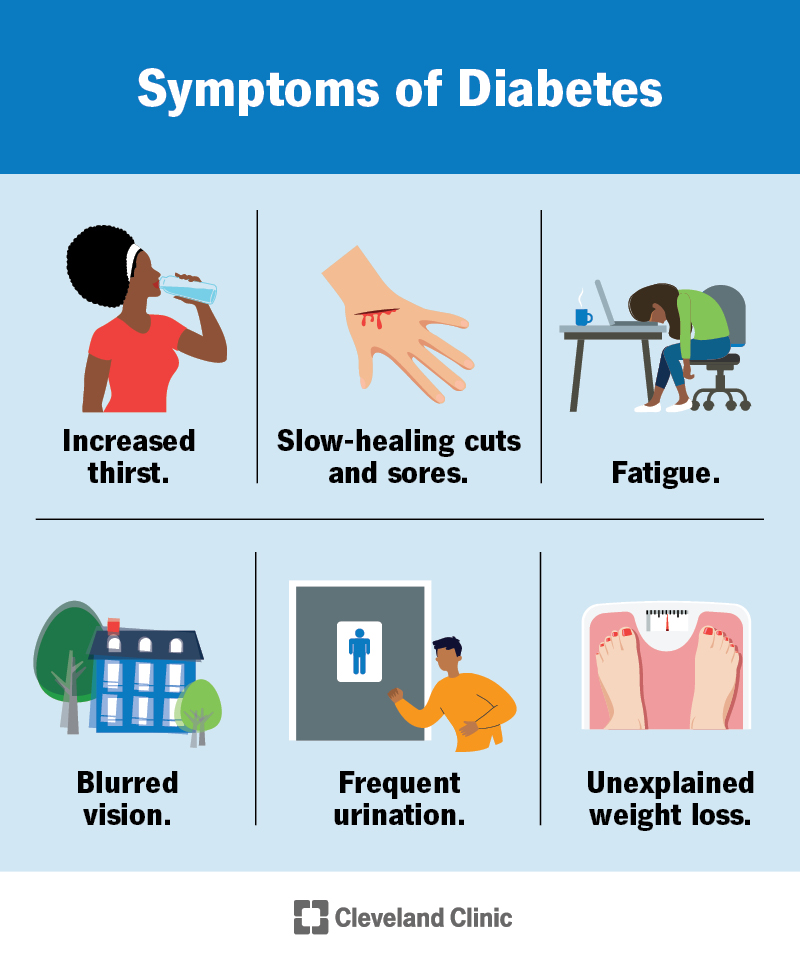
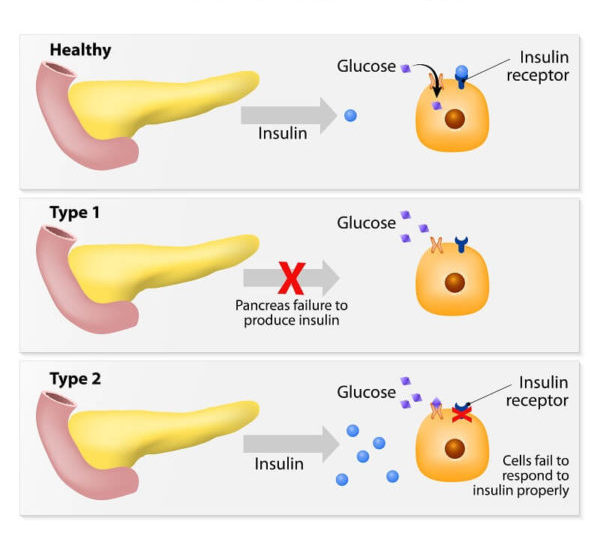
Diabetes is a chronic medical condition characterized by high levels of blood sugar (glucose). This occurs either because the body doesn’t produce enough insulin (a hormone that regulates blood sugar) or because the cells don’t respond properly to the insulin that is produced. Insulin is necessary for the body to effectively use glucose as a source of energy.
History for diabetes mellitus type 1 and 2:
Symptoms of hyperglycemia
Thirst, dry mouth
Polyuria
Nocturia
Tiredness, fatigue, lethargy
Noticeable change in weight (usually weight loss)
Blurring of vision
Pruritus vulvae, balanitis (genital candidiasis)
Nausea; headache
Hyperphagia; predilection for sweet foods
Mood change, irritability, difficulty in concentrating, apathy
Family history
Physical examination for diabetes mellitus type 1 and 2
BMI
Retinal examination
Orthostatic blood pressure
Foot examination
Peripheral pulses
Insulin injection sites
Peripheral neuropathy
Type 1 Vs Type 2 Diabetes mellitus DM
Type 1
Type 2
Onset
Sudden
Gradual
Age at onset
Any (mostly young)
Mostly in adults
Body habitus
Thin or normal
Often obese
Ketoacidosis
Common
Rare
Autoantibodies
Usually +
Absent
Endogeneous insulin
Low or absent
Normal, decreased or increased
Concordance in identical twins
~ 50%
~90%
Prevalence
Less prevalent
More prevalent (~90-95% of US diabetics)
Biochemical
C-peptide disappears
C-peptide persists
Increased bloog glucose sugar level definition is called when
Two-hour glucose during OGTT <140 mg/dL (7.8 mmol/L)
Categories of increased risk for diabetes:
•Impaired fasting glucose(IFG)
FPG between 100 and 125 mg/dL (5.6 to 6.9 mmol/L).
•Impaired glucose tolerance(IGT)
Two-hour – 75 g OGTT between 140 and 199 mg/L (7.8 to 11.0 mmol/L).
•A1C – Persons with 5.7 to 6.4 percent (39 to 46 mmol/mol
Diagnostic criteria of Diabetes mellitus
1. A1C ≥6.5 percent OR 2. Fasting Plasma Glucose ≥126 mg/dL (7.0 mmol/L) (Fasting is defined as no caloric intake for at least eight hours.) OR 3. Two-hour plasma glucose ≥200 mg/dL (11.1 mmol/L) during an OGTT. (The test should be performed using a glucose load containing the equivalent of 75-gram anhydrous glucose dissolved in water.) OR 4. In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose ≥200 mg/dL (11.1 mmol/L).
1. A1C ≥6.5 percent
OR
2. Fasting Plasma Glucose ≥126 mg/dL (7.0 mmol/L)
(Fasting is defined as no caloric intake for at least eight hours.)
OR
3. Two-hour plasma glucose ≥200 mg/dL (11.1 mmol/L) during an OGTT.
(The test should be performed using a glucose load containing the equivalent of 75-gram anhydrous glucose dissolved in water.)
OR
4. In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose ≥200 mg/dL (11.1 mmol/L).
Advice to patients with Impaired glucose tolerance
Have an increased risk both of progression to type 2 diabetes and of developing macrovascular disease
Advice lifestyle modification reduces the risk of progression in IGT
Monitor annually by measurement of fasting blood glucose
Other cardiovascular risk factors treate aggressively
Swasthya Sewa Niyamawali 2053 is a set of health service regulations implemented in Nepal. It outlines guidelines and standards for the provision of healthcare services in the country. The regulations cover various aspects such as health facility management, service delivery, infrastructure requirements, human resources, and quality assurance. The goal of the Niyamawali is to ensure the availability of quality healthcare services and protect the rights of patients. It plays a crucial role in regulating the healthcare sector and improving the overall health system in Nepal.
Summary of Swasthya sewa niyamawali 2055
Here are some additional facts about Swasthya Sewa Niyamawali in Nepal:
Development and Implementation: Swasthya Sewa Niyamawali 2055 was developed by the Government of Nepal in collaboration with health experts and stakeholders. It was implemented in 1996 and has undergone subsequent revisions to address evolving healthcare needs.
Coverage: The Niyamawali applies to a wide range of health facilities, including hospitals, clinics, nursing homes, dispensaries, and health posts. It ensures that both public and private health institutions adhere to the prescribed standards.
Service Delivery: The regulations define the responsibilities and obligations of healthcare providers in delivering services. It covers areas such as patient care, emergency services, referral mechanisms, pharmaceutical services, and preventive measures.
Infrastructure Requirements: The Niyamawali sets forth standards for infrastructure and physical facilities. It includes provisions for hygiene, sanitation, waste management, medical equipment, and adequate space for patient care.
Human Resources: The regulations address the requirements for healthcare professionals, including qualifications, licensing, and registration. It emphasizes the need for qualified medical personnel and skilled staff in health facilities.
Quality Assurance: Swasthya Sewa Niyamawali emphasizes the importance of quality assurance in healthcare. It establishes mechanisms for monitoring, evaluation, and accreditation of health services to ensure compliance with defined standards.
Patient Rights and Safety: The Niyamawali places a strong emphasis on protecting the rights and safety of patients. It outlines measures to ensure confidentiality, informed consent, patient education, and handling of complaints and grievances.
Capacity Building and Training: The regulations promote continuous capacity building and professional development of healthcare providers. It encourages training programs, workshops, and research to enhance the skills and knowledge of medical personnel.
Enforcement and Penalties: Swasthya Sewa Niyamawali empowers regulatory bodies to enforce compliance with the regulations. It outlines penalties and legal consequences for non-compliance, including fines, suspension, or revocation of licenses.
Ongoing Revisions: The Niyamawali is periodically reviewed and revised to align with emerging healthcare needs and advancements. This ensures that the regulations remain relevant and effective in addressing the evolving healthcare landscape in Nepal.
swasthya sewa niyamabali 2055 download below:
Summary of swasthya sewa niyamawali:
Swasthya Sewa Niyamawali 2055 is a set of health service regulations implemented in Nepal. It outlines guidelines and standards for the provision of healthcare services in the country. The regulations cover various aspects such as health facility management, service delivery, infrastructure requirements, human resources, and quality assurance.
The goal of the Niyamawali is to ensure the availability of quality healthcare services and protect the rights of patients. It plays a crucial role in regulating the healthcare sector and improving the overall health system in Nepal.
Thank you.
Stay Connected with Dr. Chaitanya Joshi, MD
YouTube Channel
Watch health videos, tips, and updates from Dr. Chaitanya MD.