Introduction of dyspenea: what is dyspena or shortness of breath
What is dyspnea?
Shortness of breath causes and ddx?
Table of contents(toc)
Introduction of dyspnoea
Dyspena is a condition in which a person feels difficulty breathing.
It is a subjective experience expressed by the patient. The casuse or origin of this may come formvarying reasons including physiological, psychological, social, and environemntal factors.
Thus produced discomfort now is tackled by our physiological response as change in physiological parameters or behavioral modofications including shortnes of breathing.
Dyspnoea can be classified as acute or chronic.
Acute dyspnoea develops withing hours to days while chronic develops over weeks to lnger duration. The causes of acute and chronic dyspnoea might be different depending upon the duration.
Pulse oxymeter
After careful history taking and examination of the patient having dyspnoea we should make a good list of differential disagnoses. The various differential diagnoses of dyspnoea are summerized in the following list.
The source of causes dyspnea, shortness of breath can be listed as:
Cardiovascular and realted to use of oxygen
Resporatory and chest wall pathology
Psychogenic
Differential diagnoses of dyspnoea/shortness of breath:
1. Causes of acute SOB
Cardiovascular
Cardiogenic
Impaired oxygen delivery
Impaired oxygen use
Respiratory causes
Upper airway
Lower aiway causes
Psychogenic
panic disorder
conversion disorder
drug withdrawal
2. Causes of Chronic SOB
Cardiovascular cause
CHF
Pericarditis
Anemia
Respiratory causes
Pathologies of chest wall, bronchoalveolar system, airways and lung parenchyma
The diseases can be summarised as below:
1. Cardiovascular
Acute MI
CHF/ LH failure
Aortic/Mitral stenosis
Aortic/Mitral Regurgitation
Arrhythmia
Cardiac tamponade
Constrictive pericarditis
Left sided obstructive lesions (atrial myxoma)
Elevated pulmonary venous pressure
2. Respiratory
i) Airway
Asthma
COPD
Upper airway obstruction like foreign body, anaphylaxis, mucus plugging
नेपाल को खोप तालिका बारे छोटो जानकारी (Rastriya Khop talika Nepal)
नेपालमा बच्चा जन्मे देखि दुई वर्षको उमेर सम्म विभिन्न १३ रोग विरुद्धको खोप निःशुल्क लगाइन्छ।
यी खोपहरु सरकारी स्वास्थ्य संस्था हरु मा निःशुल्क पाइन्छ।
गर्भवती महिला लाई दुई डोज टिटानस विरुद्ध को खोप निःशुल्क लगाइन्छ।
कुकुर र रेबिज सार्न सक्ने जनावरले तोकेको व्यक्तिलाई समेत रेबिज विरुद्धको खोप विभिन्न संस्थाहरुमा निःशुल्क लगाइन्छ।
BCG vaccinating a child; SC subcuticular
खोप बारे विशेष जानकारी vaccine information
अहिले नेपाल सरकारले माथि उल्लेखित अवधिमा खोप लगाउन छुटेका बालबालिकाहरूलाई समेत खोप लगाएर रोगहरू बाट जोगाउन पांच वर्षको उमेरका बच्चा हरु लाई समेत खोप लगाउने निर्णय गरेको छ।
यो खोप वैशाख १५ र ३१ गते नेपाल सरकार अन्तर्गत का स्वास्थ्य संस्था हरु मा निःशुल्क लगाइन्छ।
दुई वर्ष को उमेर सम्म खोप लगाइसकेका बच्चा हरु लाई यो अवधिमा थप खोप लगाउन आवश्यक छैन।
खोप लगाउन किन जरुरी छ? Why is vaccine important in Nepal
खोपले बालबालिका हरु लाई १३ थरी रोगहरूबाट जोगाउँछ। यो रोगहरू निम्नानुसार छन्।
MCQs regarding Pulmonary tuberculosis Health exams preparation
Introduction
I hope you are doing well and reading this. As you are aware, we will be using Google Forms to administer an upcoming multiple-choice test. I’m writing to respectfully ask that you take the test and do your best.
Tips and tricks
It is quick and easy to gauge your level of subject knowledge by taking the test using Google Forms. As many tests are now taken online, it’s also a fantastic chance to practice test-taking techniques.
Before you proceed…
Before beginning the test, please be sure you read and comprehend the instructions and to have a reliable internet connection. Please do not hesitate to contact me for help if you run into any technical issues.
MCQ on Pulmonary tuberculosis Google forms
Final Note on PTB
Please comment your score below
Thank you for your submision.
Tags(please ignore): Health exams Exam preparation Medical exams Health test Study tips Health education Health knowledge Exam stress Health science Health information Exam strategies Health conditions Test anxiety Health promotion Exam resources Health resources Health research Exam techniques Health coaching Exam success PSC exam preparation Lok Sewa exam tips License exam study material Exam syllabus Exam pattern Previous year question papers Mock exams General knowledge for exams Exam eligibility criteria Exam registration Exam dates Exam centers Exam results Exam analysis Exam cutoff marks Exam books and guides Exam coaching Exam time management Exam revision techniques Exam success stories Public service commission exam Civil service exam preparation PSC exam syllabus PSC exam pattern PSC exam eligibility PSC exam registration PSC exam dates PSC exam centers PSC exam results PSC exam preparation tips Lok Sewa Aayog exam preparation Lok Sewa Aayog exam syllabus Lok Sewa Aayog exam pattern Lok Sewa Aayog exam eligibility Lok Sewa Aayog exam registration Lok Sewa Aayog exam dates Lok Sewa Aayog exam centers Lok Sewa Aayog exam results License exam preparation License exam syllabus License exam pattern License exam eligibility License exam registration License exam dates License exam centers License exam results License exam preparation tips General knowledge for PSC, Lok Sewa, and license exams Current affairs for exams Mental ability for exams
Nursing care for pleural effusion and chest tube inserted patient
Observe for infection, local inflammation
Check dressing
Check if tube is blocked
Mobilization care
Check for amount and color of drainage
Pain management
Ensure breathing and lung reexpansion in case of collapse
Prevent clamping
Ensure positioning
References
Davidson’s Principles and Practice of Medicine 21st edition
Harrison’s Principle of Internal Medicine, 18th edition
MCQs related to pleral effusion:
What is pleural effusion?
a) Accumulation of air in the pleural space
b) Collection of fluid in the pleural space
c) Infection of the pleural cavity
Answer: b) Collection of fluid in the pleural space
What is pneumothorax?
a) Collection of fluid in the pleural space
b) Accumulation of air in the pleural space
c) Infection of the pleural cavity
Answer: b) Accumulation of air in the pleural space
Which condition is more likely to cause chest pain?
a) Pleural effusion
b) Pneumothorax
c) Both conditions can cause chest pain
Answer: c) Both conditions can cause chest pain
Which condition is more likely to cause shortness of breath?
a) Pleural effusion
b) Pneumothorax
c) Both conditions can cause shortness of breath
Answer: c) Both conditions can cause shortness of breath
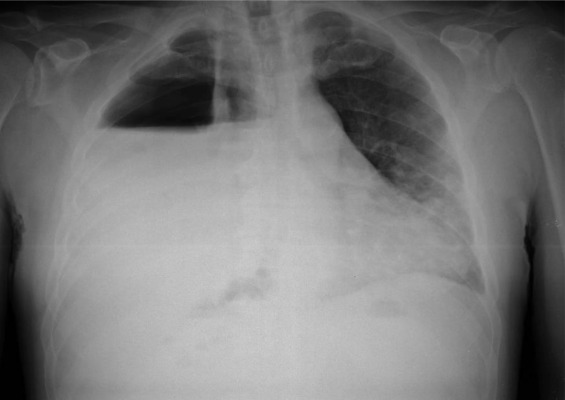
Which of the following imaging studies is most commonly used to diagnose pleural effusion?
a) Chest x-ray
b) Computed tomography (CT)
c) Magnetic resonance imaging (MRI)
Answer: a) Chest x-ray
Which of the following conditions can be diagnosed by thoracentesis?
a) Pleural effusion
b) Pneumothorax
c) Both conditions can be diagnosed by thoracentesis
Answer: a) Pleural effusion
Which of the following imaging studies is most commonly used to diagnose pneumothorax?
a) Chest x-ray
b) Computed tomography (CT)
c) Magnetic resonance imaging (MRI)
Answer: a) Chest x-ray
Which of the following conditions can be treated with a chest tube?
a) Pleural effusion
b) Pneumothorax
c) Both conditions can be treated with a chest tube
Answer: c) Both conditions can be treated with a chest tube
What is the primary treatment for small, uncomplicated pneumothorax?
a) Observation
b) Chest tube insertion
c) Surgery
Answer: a) Observation
What is the primary treatment for large, complicated pneumothorax?
a) Observation
b) Chest tube insertion
c) Surgery
Answer: b) Chest tube insertion
Which of the following is a potential complication of pleural effusion?
a) Respiratory failure
b) Cardiac arrest
c) Seizures
Answer: a) Respiratory failure
Which of the following is a potential complication of pneumothorax?
a) Respiratory failure
b) Cardiac arrest
c) Seizures
Answer: a) Respiratory failure
Which of the following conditions is more common in individuals with chronic obstructive pulmonary disease (COPD)?
a) Pleural effusion
b) Pneumothorax
c) Both conditions are equally common in individuals with COPD
Answer: b) Pneumothorax
Which of the following conditions is more common in individuals with heart failure?
a) Pleural effusion
b) Pneumothorax
c) Both conditions are equally common in individuals with heart failure
Answer: a) Pleural effusion
What is the most important factor in determining the severity of pneumothorax?
a) The size of the pneumothorax
b) The cause of the pneumothorax
c) The location of the pneumothorax
Answer: a) The size of the pneumothorax
✌
Tags(please ignore): Health exams Exam preparation Medical exams Health test Study tips Health education Health knowledge Exam stress Health science Health information Exam strategies Health conditions Test anxiety Health promotion Exam resources Health resources Health research Exam techniques Health coaching Exam success PSC exam preparation Lok Sewa exam tips License exam study material Exam syllabus Exam pattern Previous year question papers Mock exams General knowledge for exams Exam eligibility criteria Exam registration Exam dates Exam centers Exam results Exam analysis Exam cutoff marks Exam books and guides Exam coaching Exam time management Exam revision techniques Exam success stories Public service commission exam Civil service exam preparation PSC exam syllabus PSC exam pattern PSC exam eligibility PSC exam registration PSC exam dates PSC exam centers PSC exam results PSC exam preparation tips Lok Sewa Aayog exam preparation Lok Sewa Aayog exam syllabus Lok Sewa Aayog exam pattern Lok Sewa Aayog exam eligibility Lok Sewa Aayog exam registration Lok Sewa Aayog exam dates Lok Sewa Aayog exam centers Lok Sewa Aayog exam results License exam preparation License exam syllabus License exam pattern License exam eligibility License exam registration License exam dates License exam centers License exam results License exam preparation tips General knowledge for PSC, Lok Sewa, and license exams Current affairs for exams Mental ability for exams
Smoking and alcohol use? the benefits of smoking and the harms of smoking?
Table of Contents(toc)
Introduction
Smoking and alcohol use are two of the most prevalent and dangerous health risks in the world today. Both habits can have a devastating impact on a person’s physical and mental health, leading to a wide range of diseases and conditions that can be life-threatening.
The Harms of Smoking
There are several harms of smoking that include personal, health, family , social and nation wise harms. It not only harms teh user but also the whole bnation and the global effect is there.
Effect of smoking
Cigarette smoking is a leading cause of preventable death worldwide. Smoking can cause a wide range of health problems, including lung cancer, heart disease, stroke, and chronic obstructive pulmonary disease (COPD). Smoking also affects the reproductive system, leading to fertility issues in both men and women. It can also harm unborn babies, causing low birth weight and a range of other problems.
No Smoking
Smoking and lung cancer
One of the most significant risks of smoking is lung cancer. According to the American Lung Association, smoking causes 85% of lung cancer cases in the United States. In addition to lung cancer, smoking can also cause other types of cancer, including throat, bladder, and pancreatic cancer. Smoking can also lead to emphysema, a condition in which the air sacs in the lungs are damaged, making it difficult to breathe.
Cardiovascular risks of smoking
Smoking also damages the cardiovascular system, increasing the risk of heart attack and stroke. Nicotine in tobacco smoke raises blood pressure and heart rate, while carbon monoxide reduces the amount of oxygen that can be carried in the blood, making it more difficult for the heart to pump blood. The Harms of Alcohol Use
Alcohol use is also a significant health risk, particularly when consumed in excess. Alcohol consumption can cause liver disease, pancreatitis, and a range of other health problems. Chronic alcohol use can also lead to high blood pressure, heart disease, and stroke.
Excessive alcohol use can also lead to alcoholism, a condition in which a person becomes physically and psychologically dependent on alcohol. Alcoholism can lead to a range of problems, including social isolation, relationship issues, and financial difficulties.
Alcohol drinks
Physical health risks of smoking
In addition to the physical health risks, alcohol use can also have a significant impact on mental health. Alcohol use can increase the risk of depression and anxiety, and it can also lead to other mental health problems, such as bipolar disorder.
No smoking sign
Conclusion
Beer in a glass
Smoking and alcohol use are two of the most significant health risks facing people today. Both habits can have a devastating impact on a person’s physical and mental health, leading to a wide range of diseases and conditions that can be life-threatening. If you smoke or drink alcohol, it is important to take steps to quit or reduce your use. Talk to your healthcare provider for guidance and support on quitting smoking and cutting back on alcohol use. Your health and well-being are too important to risk.
Comprehensive Abortion Care (CAC) is a patient-centered, comprehensive approach to abortion that includes services ranging from counseling and medical procedures to post-abortion care and support. It prioritizes women’s health, safety, and well-being while protecting their reproductive rights. CAC addresses not only the medical elements of abortion, but also the social, emotional, and psychological issues that influence a woman’s decision-making process. This article discusses the significance of comprehensive abortion treatment and its components.
Understanding Comprehensive Abortion Care
Abortion Care that is Comprehensive goes beyond the typical focus on medical procedures. It recognizes that women’s needs and experiences vary, and that these must be taken into account while providing abortion services. CAC’s basic components are as follows:
Safe and Legal Abortion Services:
CAC guarantees that women have safe and legal abortion methods available to them. Abortions are performed in a clinical setting by qualified healthcare professionals in accordance with medical standards and guidelines. Legal frameworks must protect women’s right to choose abortion without fear of legal prosecution.
Pre-Abortion Counseling:
Proper counseling is crucial to ensure that women make informed decisions about their reproductive health. It involves providing accurate information about abortion methods, potential risks, and available support services. Counseling also addresses emotional and psychological concerns, helping women feel confident in their choices.
Medical Procedures:
Proper counseling is essential to ensuring that women make educated reproductive health decisions. It entails disseminating correct information regarding abortion methods, dangers, and available support services. Counseling also tackles emotional and psychological issues, allowing women to feel more confidence in their decisions.
Comprehensive care goes beyond the actual abortion. Follow-up consultations to check on physical healing and treat any issues are part of post-abortion care. To assist women in overcoming any potential emotional difficulties, counseling and emotional support are also available.
Contraceptive Services:
Access to contraceptive advice and services is a component of CAC in order to avoid future unwanted pregnancies. Based on their health, lifestyle, and reproductive objectives, this assists women in selecting an effective contraceptive technique.
Respect for Women’s Autonomy and Rights:
Women’s right to make their own decisions about their reproductive health is upheld by CAC. It acknowledges that every woman has a special situation, and that her decisions should be respected without bias or pressure.
Importance of Comprehensive Abortion Care
Here is teh importance of CAC explained in detail.
Promoting Women’s Health and Well-being:
Women’s health and safety are given top priority by CAC, lowering the likelihood of unsafe and unauthorized abortions. Abortion is a safe medical procedure with few risks when done by qualified specialists.
Reducing Maternal Mortality and Morbidity:
Abortions performed unsafely play a substantial role in maternal mortality and morbidity rates around the world. By guaranteeing that women have access to secure abortion services, CAC plays a crucial part in lowering these dangers.
(ads1)
Supporting Reproductive Rights:
An essential reproductive right is the availability of comprehensive abortion care. Women are given more control over their bodies and destinies thanks to CAC, which promotes gender equality and women’s empowerment.
Addressing Stigma and Emotional Well-being:
The emotional and psychological effects of abortion are acknowledged by CAC. It aids women in overcoming any stigma or emotional difficulties they may experience by offering counseling and support.
Preventing Unintended Pregnancies:
Contraceptive services are a part of CAC, which supports family planning and reproductive health by assisting women in preventing future unplanned pregnancies.
Happy family
Conclusion
Comprehensive abortion care includes counseling, support, and empowerment in addition to medical treatments. It is a comprehensive strategy that defends women’s rights, respects their autonomy, and advances their health. To protect women’s health, lower maternal mortality, and advance reproductive justice, access to CAC must be ensured. In order to guarantee that women have the support and tools they need to make educated decisions about their reproductive health, it is critical to promote and emphasize comprehensive abortion care as societies change.
जुका एक परजीवी जनावरको संक्रमणले गर्दा पेटमा हुने समस्या हो।
जुकालाई अङ्ग्रेजीमा राउण्ड वर्म “round worm” भनिन्छ। यो aschelminthes ग्रुपमा पर्ने एक परजीवी हो। जुकाले पेटमा गएर आन्द्राको भित्री भागमा घाउ बनाउँछ र त्यहाँबाट रगत र पौष्टिक तत्व चुस्ने गर्दछ।
Juka ko symptoms जुकाका लक्षणहरू
सुरुसुरुमा जुका परेको बेला कुनै पनि लक्षण नदेखिन सक्छन्। बिस्तारै पेट बाउँडिने, वाकवाकी लाग्ने, बान्ता आउने, खाना नपच्ने, पखाला लाग्ने आदि लक्षण देखिन सक्छन्।
धेरै जुका परेको खण्डमा यी लक्षण झनै कडा हुन्छन् र कहिलेकाहीं आन्द्रा बन्द हुने र अपरेसन गर्न पर्ने अवस्था समेत आउन सक्छ।
Juka
pet ma juka parnu पेटमा जुका पर्नुका लक्षणहरु:
पेटमा जुका पर्नुको अर्थ आन्द्रामा जुका पर्नु हो। जुका फोहोर हात, खानेकुराबाट सरेर मानिसको मुखमा पुग्छ र निलिएर पेट सम्म पुग्छ। यदि सो जुका को अण्डा पेटको पाचन प्रणालीले मार्न सकेन भने त्यो आन्द्रामा पुग्छ र त्यहा बढ्न थाल्छ। त्यसपछि लक्षणहरु देखा पर्दछन।
Juka in stomach symptoms, symptoms of juka जुकाका लक्षणहरु
जुका परेमा निम्न लक्षणहरु देखा पर्न सक्छन:
पेट दुख्ने
वा्न्ता आउने, वाकवाकि लाग्ने
पखाला लाग्ने
खाना नरुच्ने
कब्जियत हुने
बच्चको केसमा, रुने, कराउने
कमजोरि हुने
थकान महसुस हुने
खाना नपच्ने
रगतको कमि हुने
Juka ko aushadhi, juka ko dabai
जुका लागेको भएमा डाक्टरले तलका मध्ये कुनै औषधि दिन सक्नुहुन्छ:
Albendazoole
Mebendazole
Pyrantel pamoate for pergnant ladies
Juka ko aushadhi in english
एल्बेनडाजोल, मेबेन्डाजोल र पाइरेनटल पामोएट लाई जुकाको उपचारको लागि प्रयोग गर्न सकिन्छ।
Juka ko medicine name
Albendazoole, Mebendazole, Pyrantel pamoate for pergnant ladies
Namle juka in english Called?
नाम्ले जुकालाई English मा tape worm ( टेप वोर्म) भनिन्छ।
अन्य प्रकारका जुकाहरु: Other worm types
मानव सरीरमा अन्य थुप्रै प्रकारका परजीवी जुका जस्ता प्राणीको संक्रमण हुने गर्दछ। जस्तै::
नाम्ले जुका
चुर्ना जुका
कलेजि जुका
हात्तिपाइले
अंकुसे जुका
अंग्रेजीमा:
Ascariasis
Hookworm Infection
Pinworm Infection (Enterobiasis)
Trichinosis
Tapeworm Infections
Liver Fluke Infection (Fascioliasis)
Schistosomiasis (Bilharzia)
Strongyloidiasis
Trichuriasis
Dracunculiasis (Guinea Worm Disease)
Churna juka in English called?
चुर्ना जुका लाई अंग्रेजीमा Pinworm भनिन्छ।
Stay Connected with Dr. Chaitanya Joshi, MD
YouTube Channel
Watch health videos, tips, and updates from Dr. Chaitanya MD.






")