Table of Contents
Pulsus paradoxus is demonstrated using a blood pressure cuff and stethoscope.
Step-by-Step Procedure
1. Position the Patient
- Patient should be lying supine or semi-recumbent
- Ask the patient to breathe normally
2. Inflate the BP Cuff
- Inflate the cuff 20–30 mmHg above systolic pressure
3. Slowly Deflate the Cuff
Deflate slowly at 2–3 mmHg per second while auscultating the brachial artery.
4. Identify the First Pressure
At first you will hear Korotkoff sounds only during expiration and they disappear during inspiration.
Record this pressure.
Example: 120 mmHg
Reason: During inspiration the systolic pressure falls below cuff pressure.
5. Continue Deflating
As the cuff pressure falls further, Korotkoff sounds will be heard throughout the respiratory cycle (during both inspiration and expiration).
Record this second pressure.
Example: 105 mmHg
6. Calculate Pulsus Paradoxus
Pulsus paradoxus=First pressure−Second pressure\text{Pulsus paradoxus} = \text{First pressure} – \text{Second pressure}Pulsus paradoxus=First pressure−Second pressure
Example:120−105=15 mmHg120 – 105 = 15\ mmHg120−105=15 mmHg
If >10 mmHg → Pulsus paradoxus present
Clinical Example
If:
- Sounds heard only in expiration at 118 mmHg
- Sounds heard throughout breathing at 102 mmHg
Then:118−102=16 mmHg118 – 102 = 16\ mmHg118−102=16 mmHg
→ Positive pulsus paradoxus

How to Demonstrate in Clinical Exam (Short Viva Answer)
You can say:
Pulsus paradoxus is demonstrated using a sphygmomanometer. The cuff is inflated above systolic pressure and slowly deflated. The first pressure at which Korotkoff sounds are heard only during expiration is noted. The pressure at which sounds are heard during both inspiration and expiration is then noted. The difference between these pressures is the pulsus paradoxus. A difference greater than 10 mmHg indicates pulsus paradoxus.
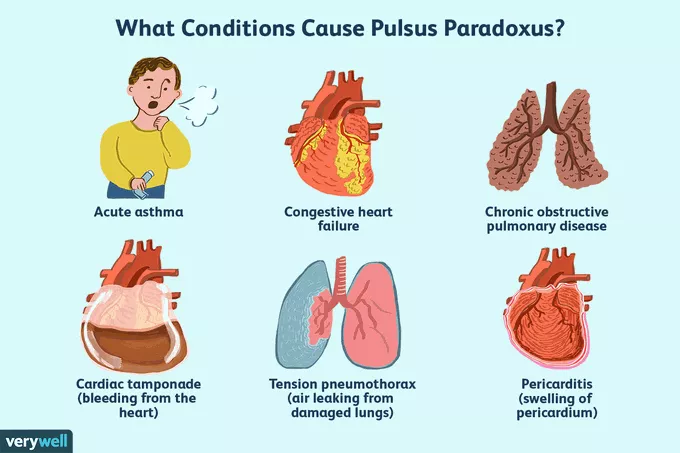
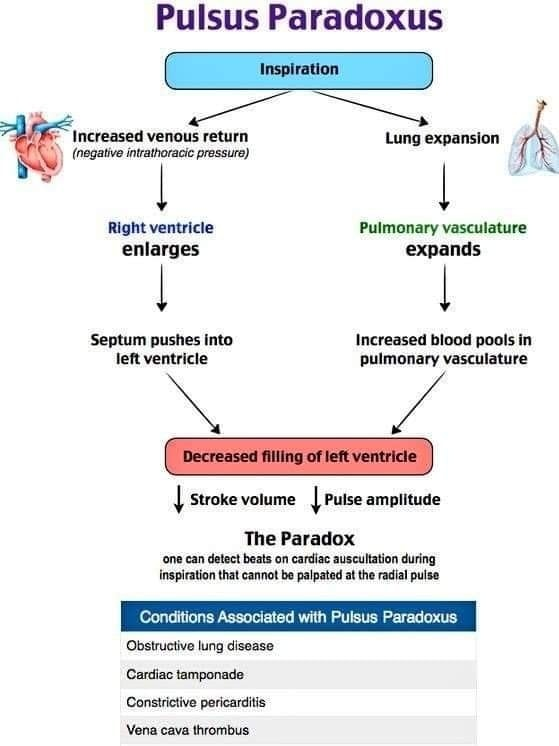
Important Clinical Associations
- Cardiac Tamponade (classic)
- Severe Asthma
- Tension Pneumothorax
- Constrictive Pericarditis
✅ Exam Tip:
If a patient has hypotension + raised JVP + pulsus paradoxus, suspect cardiac tamponade (Beck’s triad).