Enthesitis is the painful inflammation of an enthesis, the site where ligaments or tendons attach to bone. Common in spondyloarthritis (e.g., psoriatic arthritis), it typically causes pain, stiffness, and tenderness, often in the heels, elbows, or hips. Treatment includes NSAIDs, biologics, rest, and physical therapy to manage symptoms and prevent potential joint damage.
Symptoms of Enthesitis
Pain: Often described as severe or burning, specifically at tendon insertion sites, such as the Achilles tendon or bottom of the foot.
Stiffness: Increased difficulty moving the affected joint.
Tenderness: Sensitivity to touch.
Swelling: While not always present, swelling can occur in the soft tissue surrounding the site.
Impact on Mobility: Chronic cases can limit mobility and cause damage to adjacent bone and joints.
Causes and Risk Factors
Inflammatory Arthritis: Most frequently associated with psoriatic arthritis (PsA), ankylosing spondylitis (AS), and other forms of spondyloarthritis (SpA).
Physical Stress/Overuse: Repeated physical activity causing strain at the attachment site.
Immune System Dysfunction: Pro-inflammatory cytokine activity (specifically IL-17 and TNF-) is a major contributor to this inflammatory cascade.
Treatment Approaches
Medication: Non-steroidal anti-inflammatory drugs (NSAIDs) are the first line of treatment. For more chronic cases, biologics targeting TNF or IL-17 are often used.
Physical Interventions: Rest, immobilization, and gentle stretching.
Injections: Local corticosteroid injections, though used with caution near tendons.
Lifestyle Changes: Maintaining a healthy weight to reduce pressure on joints. CreakyJoints
Common Sites
Enthesitis can occur throughout the body, with more than 100 potential locations. Common sites include:
JIA = Juvenile Idiopathic Arthritis A chronic inflammatory arthritis of unknown cause beginning before age 16 and lasting ≥ 6 weeks, after exclusion of other causes.
✅ Definition (Juvenile Idiopathic Arthritis)
Arthritis in ≥1 joint
Onset < 16 years
Duration ≥ 6 weeks
Other causes excluded (infection, malignancy, trauma, connective tissue diseases)
First principle: 👉 Most overweight infants are exogenous (overfeeding). 👉 Investigations are needed only if there are red flags for endocrine, genetic, or metabolic causes.
1️⃣ Step 1: Confirm Overweight / Obesity
Anthropometry
Weight-for-length (WHO growth charts)
BMI (if >2 years; not for infants)
Head circumference
Mid-upper arm circumference (optional)
Definitions (WHO)
> +2 SD weight-for-length → Overweight
> +3 SD → Obese
2️⃣ When to Investigate?
Send investigations if:
Rapid weight gain
Short length/height (↓ linear growth)
Dysmorphic features
Developmental delay
Hypotonia
Organomegaly
Hyperphagia
Family history of endocrine/genetic disorders
Signs of hypothyroidism, Cushing, etc.
If thriving, normal length, normal development → usually no labs required.
3️⃣ Baseline Investigations (If Indicated)
Investigation
Why Send It
CBC
Baseline health
Fasting blood glucose
Insulin resistance (rare in infancy but possible in severe obesity)
Serum insulin (if strong suspicion)
Hyperinsulinemia
Lipid profile
If severe obesity or family history
LFT (ALT, AST)
NAFLD screening (rare but possible in severe cases)
Thyroid profile (TSH, Free T4)
Rule out hypothyroidism
Serum cortisol (8 AM)
If Cushing features
IGF-1
If growth failure
4️⃣ Endocrine Causes to Rule Out
A. Hypothyroidism
TSH
Free T4
Clues:
Constipation
Large tongue
Hypotonia
Poor linear growth
B. Cushing Syndrome (Very Rare in Infants)
8 AM cortisol
Low-dose dexamethasone suppression test (if needed)
Clues:
Moon face
Hypertension
Growth failure
Thin skin
C. Hyperinsulinism
Fasting insulin
Blood glucose
5️⃣ Genetic / Syndromic Evaluation
If:
Hypotonia
Developmental delay
Dysmorphism
Hyperphagia
Consider:
Karyotype
Microarray
Referral to genetics
Examples:
Prader-Willi syndrome
Beckwith-Wiedemann syndrome
6️⃣ Metabolic Screening (If Suspicion)
If:
Hepatomegaly
Hypoglycemia
Recurrent vomiting
Developmental delay
Send:
Serum ammonia
Lactate
Tandem mass spectrometry
Urine organic acids
7️⃣ If Severe Obesity (> +3 SD)
Consider screening for:
Lipid profile
LFT (NAFLD)
Blood pressure monitoring
HbA1c (if strong suspicion)
8️⃣ What NOT to Routinely Send
❌ Insulin levels in every overweight baby ❌ Extensive metabolic panels without red flags ❌ Hormone panels without growth failure
9️⃣ Practical Clinical Algorithm (Exam-Friendly)
Normal length + normal development + formula overfeeding → NO LABS
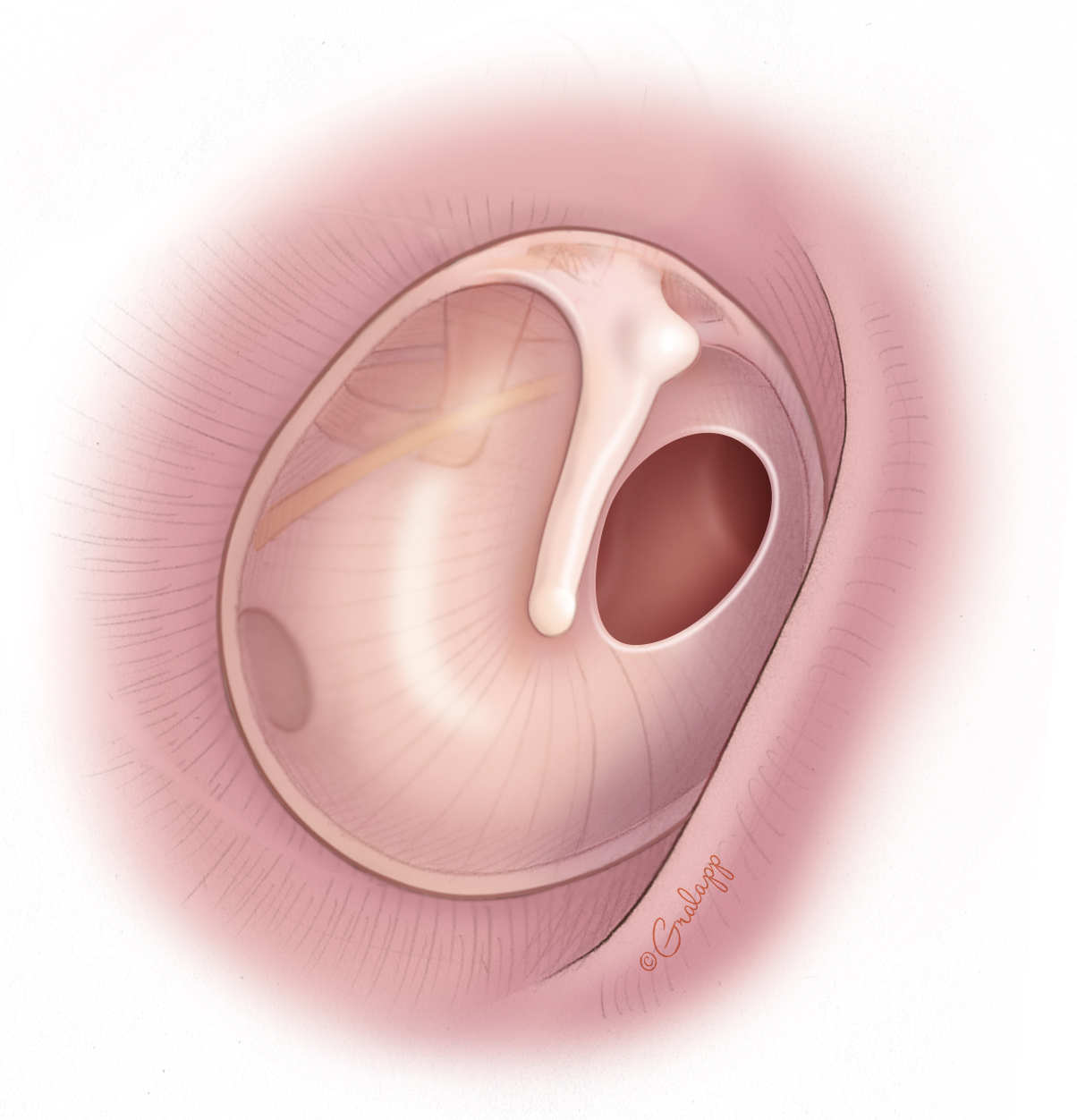
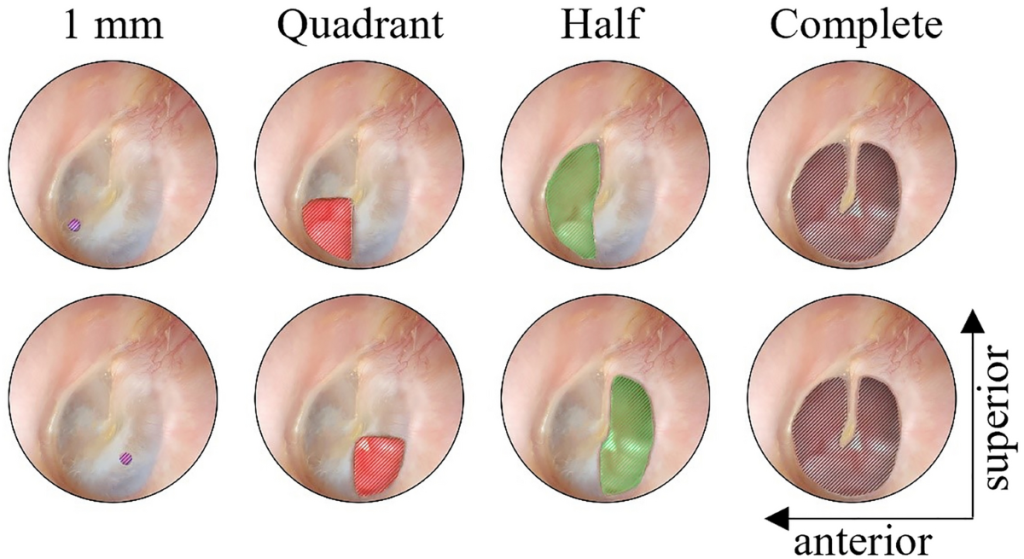
Perforated Acute Otitis Media (AOM with tympanic membrane perforation) is treated slightly differently from uncomplicated AOM because the perforation allows topical therapy to reach the middle ear.
1. First-line Treatment
A. Topical Antibiotic Ear Drops (Most Important)
Use quinolone ear drops because they are safe in perforated TM.
Ofloxacin ear drops
Dose: 5 drops in affected ear twice daily
Duration: 7–10 days
OR
Ciprofloxacin ear drops
Dose: 4–5 drops twice daily
Duration: 7–10 days
Avoid aminoglycoside drops (e.g., Gentamicin, Neomycin) because they can be ototoxic if TM is perforated.
2. Oral Antibiotics (if indicated)
Give systemic antibiotics if:
Moderate/severe infection
Fever
Young child (<2 years)
Bilateral disease
Systemic symptoms
First line:
Amoxicillin
80–90 mg/kg/day divided BID
Duration 7–10 days
If severe infection or recent amoxicillin use:
Amoxicillin‑clavulanate
90 mg/kg/day (amoxicillin component)
3. Analgesics
Paracetamol 10–15 mg/kg every 6 hours OR
Ibuprofen 10 mg/kg every 8 hours
4. Local Care
Keep ear dry (no water entry).
Do not plug ear tightly.
Gentle ear toilet/suction if discharge excessive.
5. Follow-up
Re-examine after 1–2 weeks.
Most perforations heal spontaneously within 2–4 weeks.
If persistent perforation >6 weeks → ENT referral.
Cerebral palsy (CP) is the most common cause of permanent motor disability in childhood. It results from injury or abnormal development of the immature brain, leading to abnormalities of movement, posture, and coordination.
Despite the term palsy, cerebral palsy is not a progressive disease—the brain injury is static. However, symptoms may change as the child grows.
The worldwide prevalence is approximately 2–3 per 1000 live births, and the condition is more common in premature infants and low-birth-weight neonates.
Overview of Cerebral Palsy
Definition
Cerebral palsy is defined as:
A group of permanent disorders of movement and posture causing activity limitation, attributed to non-progressive disturbances in the developing fetal or infant brain.
Key Characteristics
Feature
Description
Nature
Non-progressive brain injury
Onset
Early childhood
Primary problem
Motor dysfunction
Associated problems
Cognitive, sensory, and behavioral issues
Pathophysiology
According to First Aid for the USMLE Step 1, cerebral palsy results from injury to motor control systems of the developing brain.
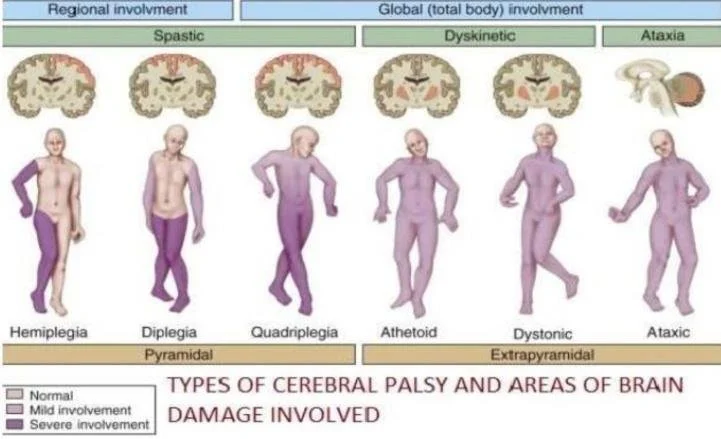
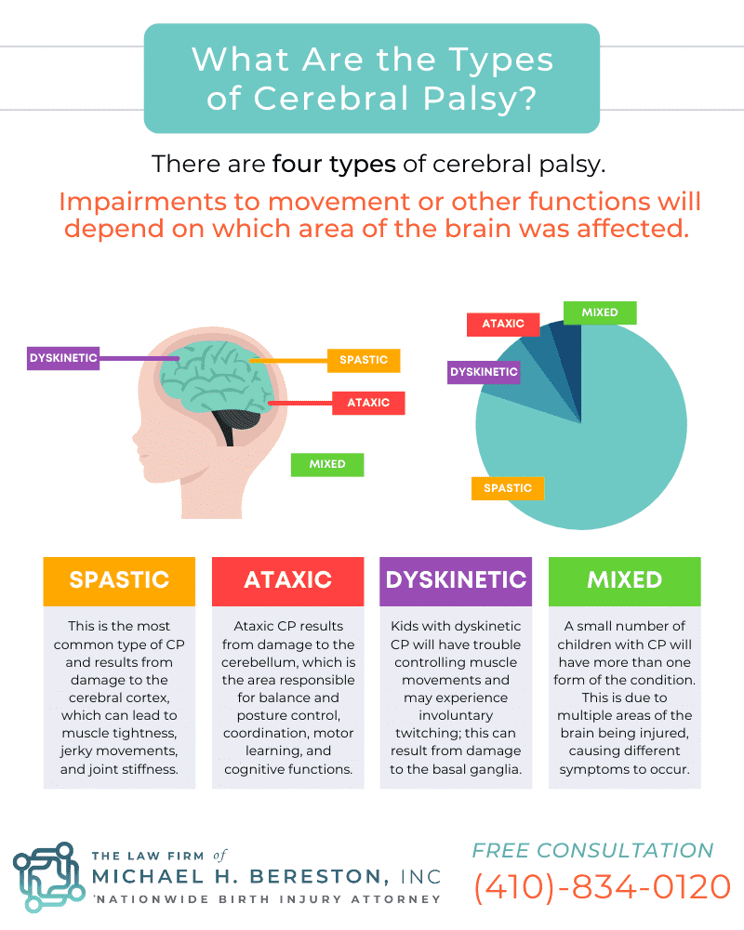
Brain Areas Involved
Brain Structure
Resulting Clinical Type
Motor cortex
Spastic CP
Basal ganglia
Dyskinetic CP
Cerebellum
Ataxic CP
Multiple regions
Mixed CP
Mechanisms of Brain Injury
Major mechanisms include:
Hypoxic-ischemic injury
White matter injury
Intracranial hemorrhage
Inflammation
Toxic injury (bilirubin toxicity)
Periventricular Leukomalacia (Common Mechanism in Preterm Infants)
Periventricular leukomalacia (PVL) is the most common neuropathologic lesion in premature infants who develop CP.
Pathogenesis
Immature cerebral circulation
Hypoxia or ischemia
White matter injury near ventricles
Damage to descending corticospinal tracts
Clinical Outcome
PVL is strongly associated with spastic diplegia.
Etiology of Cerebral Palsy
Modern research shows most CP originates before birth, rather than during delivery.
Based on Cloherty and Stark's Manual of Neonatal Care.
Maternal Factors
Neonatal Factors
Maternal infection
Prematurity
Placental insufficiency
Low birth weight
Preeclampsia
Neonatal seizures
Multiple pregnancy
Intraventricular hemorrhage
Classification of Cerebral Palsy
Types Based on Motor Pattern
Table: Major Types of Cerebral Palsy
Type
Brain Region
Key Features
Frequency
Spastic
Motor cortex
Stiff muscles, hyperreflexia
~70–80%
Dyskinetic
Basal ganglia
Involuntary movements
~6–10%
Ataxic
Cerebellum
Poor balance and coordination
~5–10%
Mixed
Multiple areas
Combination of symptoms
Variable
Spastic Cerebral Palsy
Most common type.
Pathophysiology
Damage to corticospinal tracts leads to:
Increased muscle tone
Hyperreflexia
Clonus
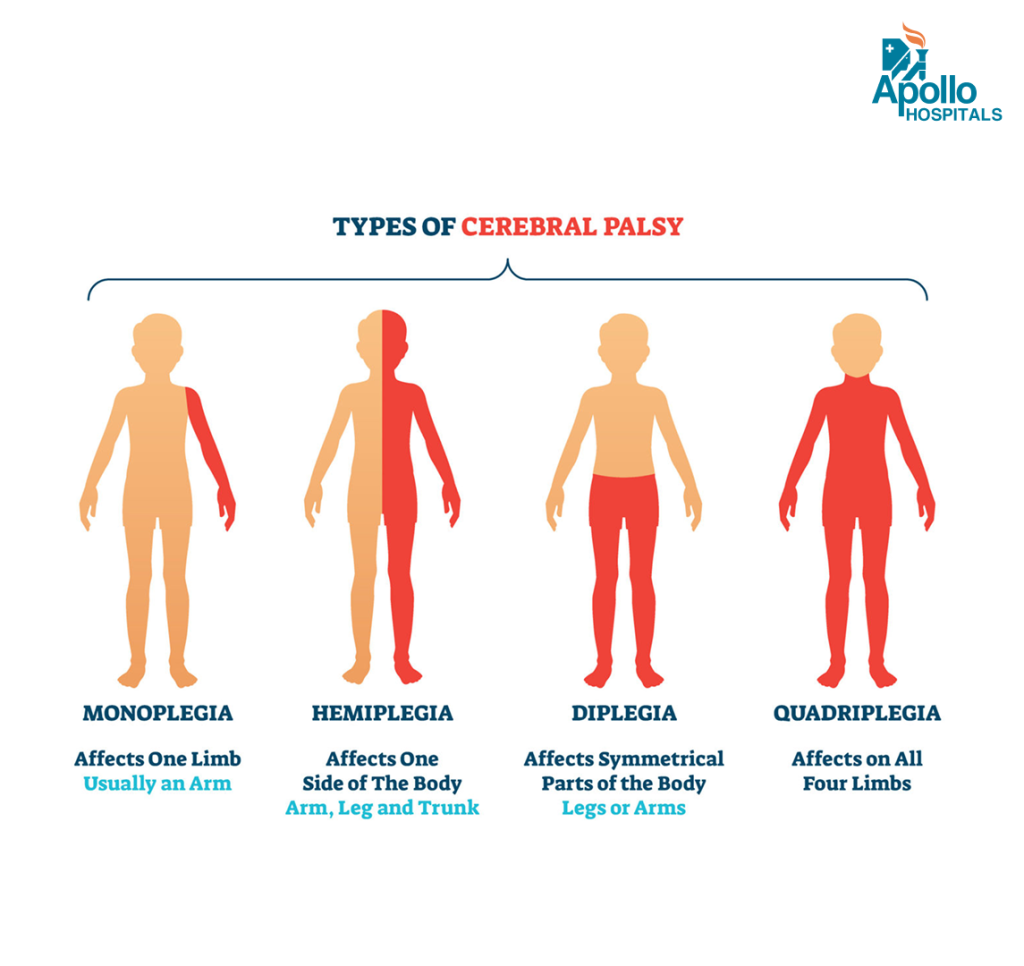
Distribution Patterns
Type
Body Areas Involved
Hemiplegia
One side of body
Diplegia
Legs > arms
Quadriplegia
All limbs
Monoplegia
Single limb
Dyskinetic Cerebral Palsy
Associated with basal ganglia injury.
Clinical Features
Dystonia
Chorea
Athetosis
Involuntary twisting movements
Important Cause
Severe neonatal jaundice causing Kernicterus.
Ataxic Cerebral Palsy
Results from cerebellar damage.
Symptoms
Symptom
Description
Ataxia
Unsteady walking
Intention tremor
Tremor during movement
Poor coordination
Difficulty performing fine motor tasks
Wide-based gait
Instability while walking
Clinical Features of Cerebral Palsy
Symptoms depend on severity and brain area affected.
Early Warning Signs
Age
Red Flag
3 months
Poor head control
6 months
Stiff or floppy muscles
9 months
Not sitting
12 months
Early hand preference
Associated Conditions
Children with CP often have additional neurological problems.
Condition
Frequency
Epilepsy
30–50%
Intellectual disability
40–60%
Visual impairment
20–40%
Speech disorders
common
Hearing loss
10–15%
Diagnosis
Diagnosis is mainly clinical, supported by imaging.
Diagnostic Evaluation
Evaluation
Purpose
Developmental history
Identify delays
Neurological exam
Tone, reflexes
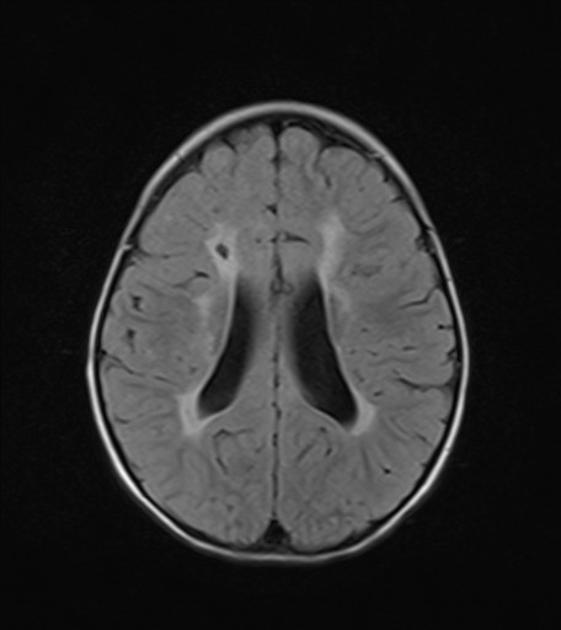
MRI brain
Identify structural lesion
EEG
If seizures present
Genetic testing
If atypical features
Neuroimaging Findings
Common MRI findings include:
Periventricular leukomalacia
Cortical malformations
Brain atrophy
Old infarction
Gross Motor Function Classification System (GMFCS)
This system classifies severity of CP.
Level
Functional Ability
Level I
Walks independently
Level II
Walks with limitations
Level III
Walks with assistive device
Level IV
Limited self mobility
Level V
Wheelchair dependent
Management of Cerebral Palsy
There is no cure, but multidisciplinary management improves function.
Multidisciplinary Treatment
Therapy
Role
Physiotherapy
Improve mobility
Occupational therapy
Daily living skills
Speech therapy
Communication
Special education
Cognitive development
Pharmacological Treatment
Used mainly for spasticity management.
Drug
Mechanism
Baclofen
GABA agonist
Diazepam
Muscle relaxant
Tizanidine
Alpha-2 agonist
Botulinum toxin
Local spasticity control
Surgical Management
Indicated in severe deformities.
Examples include:
Tendon lengthening
Hip reconstruction
Selective dorsal rhizotomy
Spinal surgery for scoliosis
Prevention Strategies
Important preventive measures include:
Strategy
Benefit
Antenatal care
Prevent infections
Prevention of prematurity
Reduce PVL
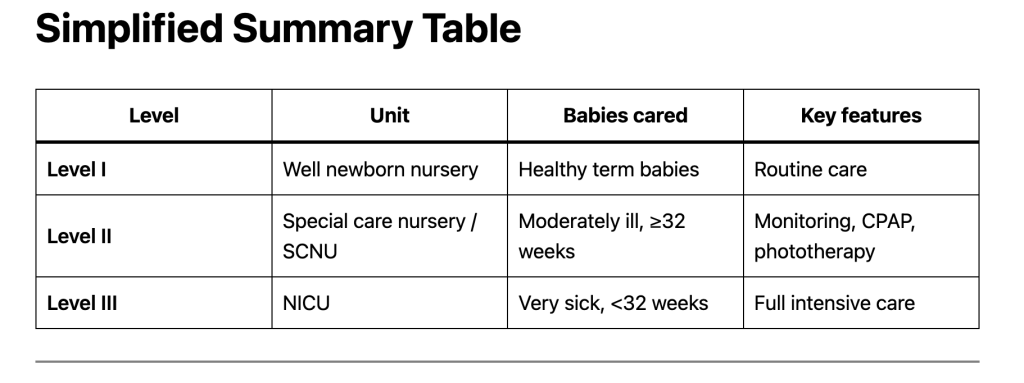
Neonatal intensive care
Prevent brain injury
Early jaundice treatment
Prevent kernicterus
Prognosis
Outcome depends on:
Severity of brain injury
Type of cerebral palsy
Associated neurological deficits
Access to rehabilitation
Many individuals with CP can live productive lives with appropriate therapy and support.
Clinical Pearls (High-Yield)
Spastic diplegia → periventricular leukomalacia
Dyskinetic CP → basal ganglia injury
Ataxic CP → cerebellar damage
Kernicterus → dyskinetic cerebral palsy
Conclusion
Cerebral palsy is a lifelong neurological disorder caused by early brain injury. Although the underlying brain damage is permanent, early diagnosis, multidisciplinary therapy, and supportive care can significantly improve functional outcomes and quality of life.
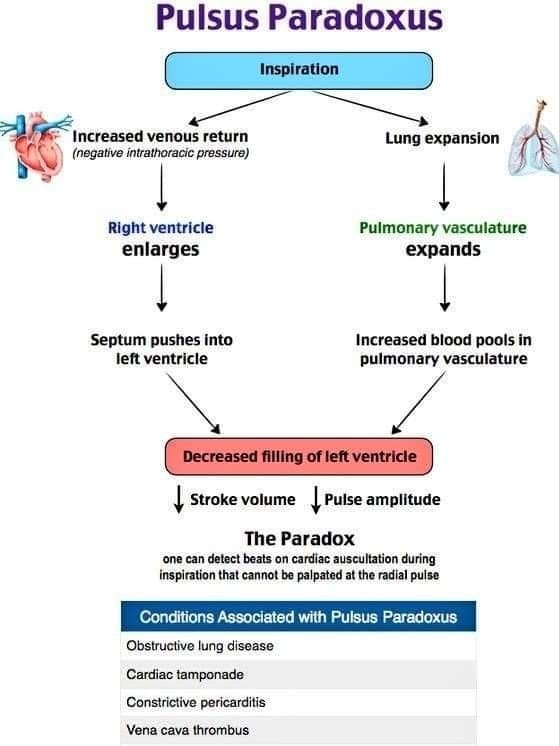
First pressure: Korotkoff sounds heard only during expiration
Second pressure: Sounds heard throughout inspiration and expiration
Difference between the two = Pulsus paradoxus
Example:
Expiration only = 120 mmHg
Throughout respiration = 105 mmHg
Pulsus paradoxus = 15 mmHg
Clinical Significance
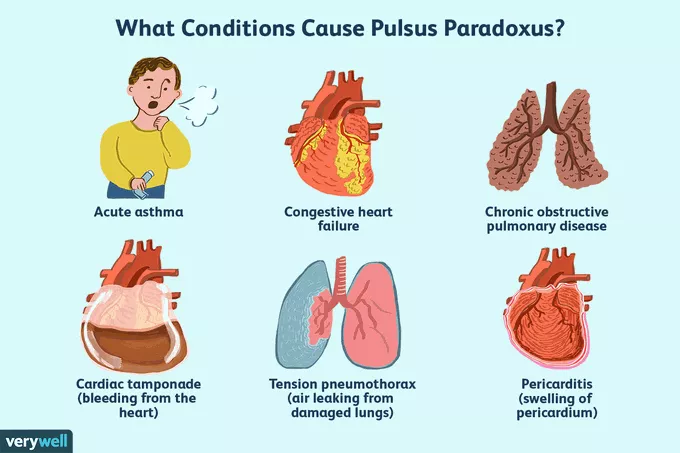
A pulsus paradoxus >10 mmHg suggests serious cardiopulmonary disease, especially:
Cardiac tamponade
Severe asthma attack
Reverse Pulsus Paradoxus
Reverse pulsus paradoxus is a rare cardiovascular finding in which systolic blood pressure increases during inspiration, opposite to the normal drop seen in typical pulsus paradoxus. It is most commonly associated with conditions that alter intrathoracic pressure dynamics or ventricular interaction, such as positive pressure ventilation, hypertrophic obstructive cardiomyopathy (HOCM), isovolumetric ventricular pacing, and sometimes aortic regurgitation.
The mechanism usually involves enhanced left ventricular filling or reduced afterload during inspiration, leading to a paradoxical rise in systolic pressure. Clinically, it is less frequently encountered than classic pulsus paradoxus and is often identified in intensive care settings where patients are mechanically ventilated. Recognition of reverse pulsus paradoxus is important because it can provide clues about underlying cardiac physiology and ventilatory influences rather than indicating conditions like cardiac tamponade, which are linked to the traditional form.
Quick Exam Definition
Pulsus paradoxus is an inspiratory fall in systolic blood pressure greater than 10 mmHg.
Stay Connected with Dr. Chaitanya Joshi, MD
YouTube Channel
Watch health videos, tips, and updates from Dr. Chaitanya MD.