

Table of Contents
- Nelson Textbook of Pediatrics
- First Aid for the USMLE Step 1
- Cloherty and Stark’s Manual of Neonatal Care
Introduction
Cerebral palsy (CP) is the most common cause of permanent motor disability in childhood. It results from injury or abnormal development of the immature brain, leading to abnormalities of movement, posture, and coordination.
Despite the term palsy, cerebral palsy is not a progressive disease—the brain injury is static. However, symptoms may change as the child grows.
The worldwide prevalence is approximately 2–3 per 1000 live births, and the condition is more common in premature infants and low-birth-weight neonates.
Overview of Cerebral Palsy




Definition
Cerebral palsy is defined as:
A group of permanent disorders of movement and posture causing activity limitation, attributed to non-progressive disturbances in the developing fetal or infant brain.
Key Characteristics
| Feature | Description |
|---|---|
| Nature | Non-progressive brain injury |
| Onset | Early childhood |
| Primary problem | Motor dysfunction |
| Associated problems | Cognitive, sensory, and behavioral issues |
Pathophysiology
According to First Aid for the USMLE Step 1, cerebral palsy results from injury to motor control systems of the developing brain.
Brain Areas Involved
| Brain Structure | Resulting Clinical Type |
|---|---|
| Motor cortex | Spastic CP |
| Basal ganglia | Dyskinetic CP |
| Cerebellum | Ataxic CP |
| Multiple regions | Mixed CP |
Mechanisms of Brain Injury
Major mechanisms include:
- Hypoxic-ischemic injury
- White matter injury
- Intracranial hemorrhage
- Inflammation
- Toxic injury (bilirubin toxicity)
Periventricular Leukomalacia (Common Mechanism in Preterm Infants)



Periventricular leukomalacia (PVL) is the most common neuropathologic lesion in premature infants who develop CP.
Pathogenesis
- Immature cerebral circulation
- Hypoxia or ischemia
- White matter injury near ventricles
- Damage to descending corticospinal tracts
Clinical Outcome
PVL is strongly associated with spastic diplegia.
Etiology of Cerebral Palsy
Modern research shows most CP originates before birth, rather than during delivery.
Causes by Timing of Brain Injury
| Timing | Causes |
|---|---|
| Prenatal | Brain malformations, infections, genetic disorders |
| Perinatal | Prematurity, birth asphyxia, intracranial hemorrhage |
| Postnatal | Infection, trauma, stroke |
Major Risk Factors
Based on Cloherty and Stark’s Manual of Neonatal Care.
| Maternal Factors | Neonatal Factors |
|---|---|
| Maternal infection | Prematurity |
| Placental insufficiency | Low birth weight |
| Preeclampsia | Neonatal seizures |
| Multiple pregnancy | Intraventricular hemorrhage |
Classification of Cerebral Palsy
Types Based on Motor Pattern

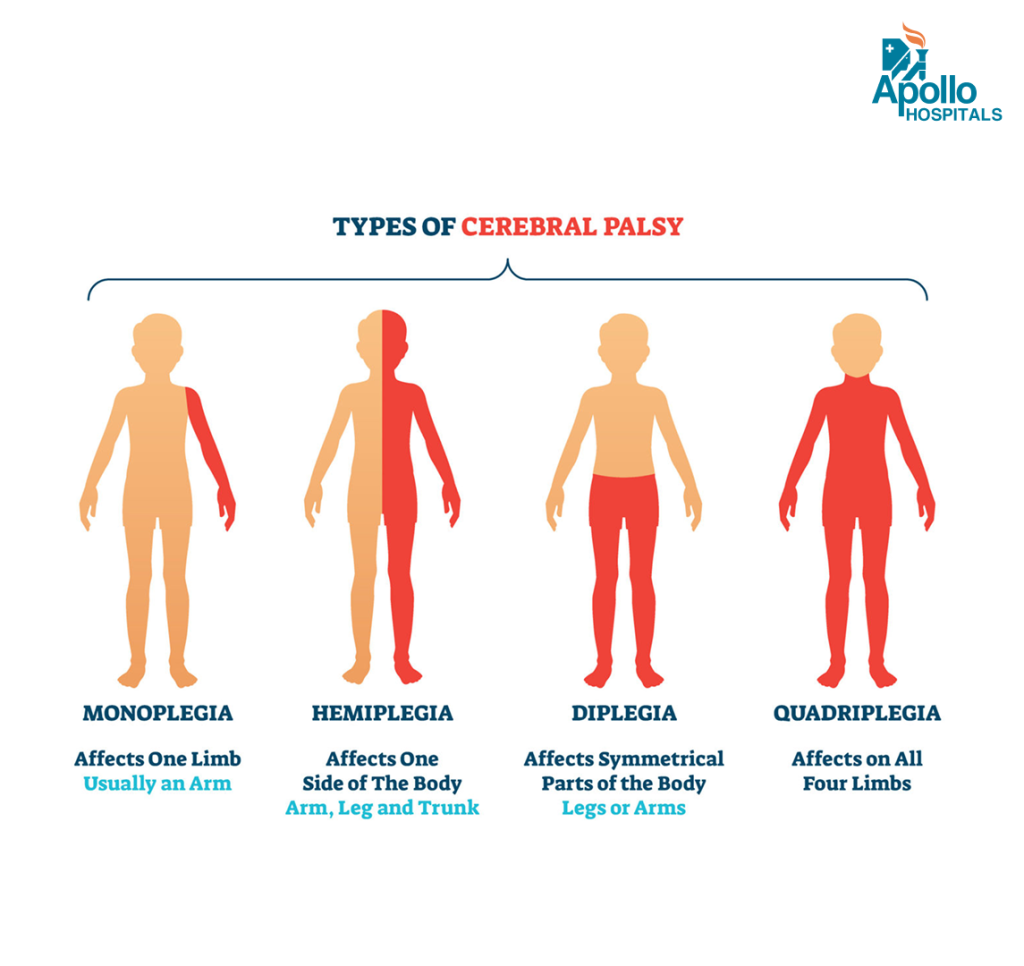
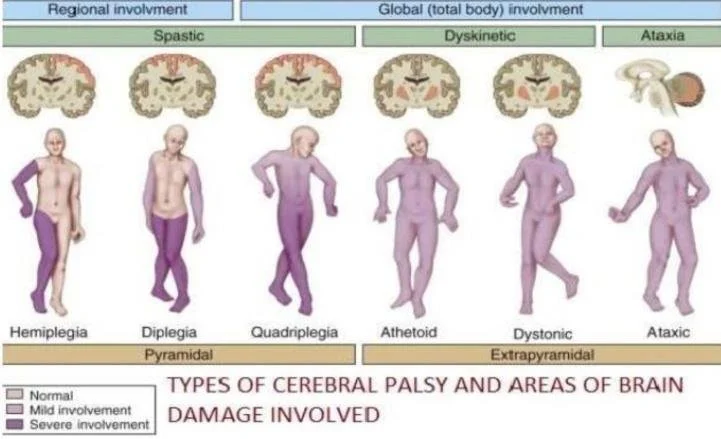

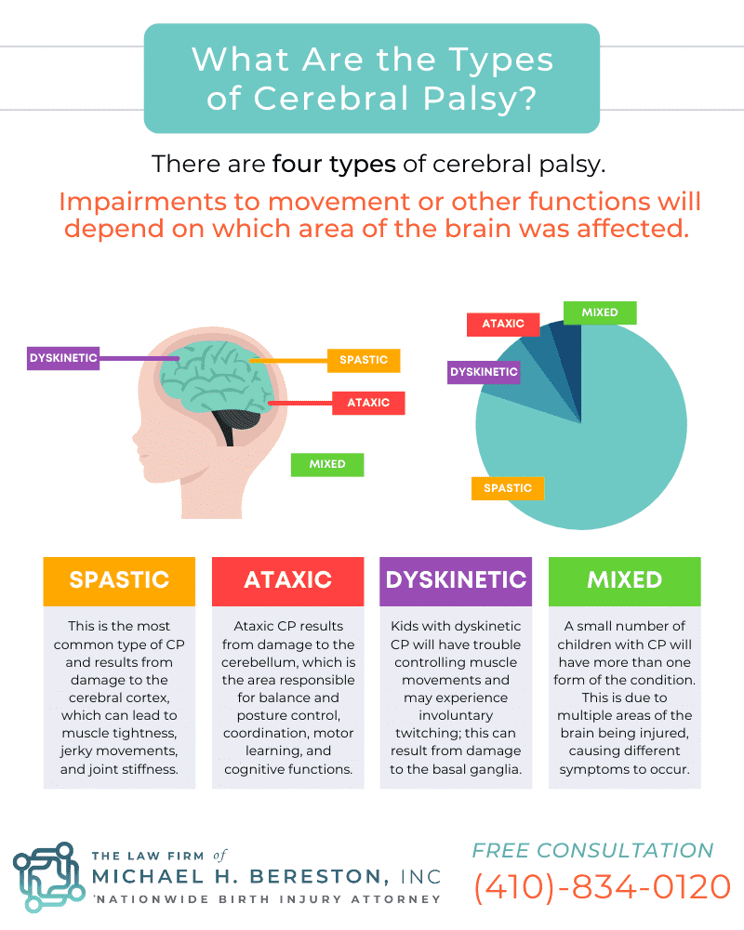
Table: Major Types of Cerebral Palsy
| Type | Brain Region | Key Features | Frequency |
|---|---|---|---|
| Spastic | Motor cortex | Stiff muscles, hyperreflexia | ~70–80% |
| Dyskinetic | Basal ganglia | Involuntary movements | ~6–10% |
| Ataxic | Cerebellum | Poor balance and coordination | ~5–10% |
| Mixed | Multiple areas | Combination of symptoms | Variable |
Spastic Cerebral Palsy
Most common type.
Pathophysiology
Damage to corticospinal tracts leads to:
- Increased muscle tone
- Hyperreflexia
- Clonus
Distribution Patterns
| Type | Body Areas Involved |
|---|---|
| Hemiplegia | One side of body |
| Diplegia | Legs > arms |
| Quadriplegia | All limbs |
| Monoplegia | Single limb |
Dyskinetic Cerebral Palsy
Associated with basal ganglia injury.
Clinical Features
- Dystonia
- Chorea
- Athetosis
- Involuntary twisting movements
Important Cause
Severe neonatal jaundice causing
Kernicterus.
Ataxic Cerebral Palsy
Results from cerebellar damage.
Symptoms
| Symptom | Description |
|---|---|
| Ataxia | Unsteady walking |
| Intention tremor | Tremor during movement |
| Poor coordination | Difficulty performing fine motor tasks |
| Wide-based gait | Instability while walking |
Clinical Features of Cerebral Palsy
Symptoms depend on severity and brain area affected.
Early Warning Signs
| Age | Red Flag |
|---|---|
| 3 months | Poor head control |
| 6 months | Stiff or floppy muscles |
| 9 months | Not sitting |
| 12 months | Early hand preference |
Associated Conditions
Children with CP often have additional neurological problems.
| Condition | Frequency |
|---|---|
| Epilepsy | 30–50% |
| Intellectual disability | 40–60% |
| Visual impairment | 20–40% |
| Speech disorders | common |
| Hearing loss | 10–15% |
Diagnosis
Diagnosis is mainly clinical, supported by imaging.
Diagnostic Evaluation
| Evaluation | Purpose |
|---|---|
| Developmental history | Identify delays |
| Neurological exam | Tone, reflexes |
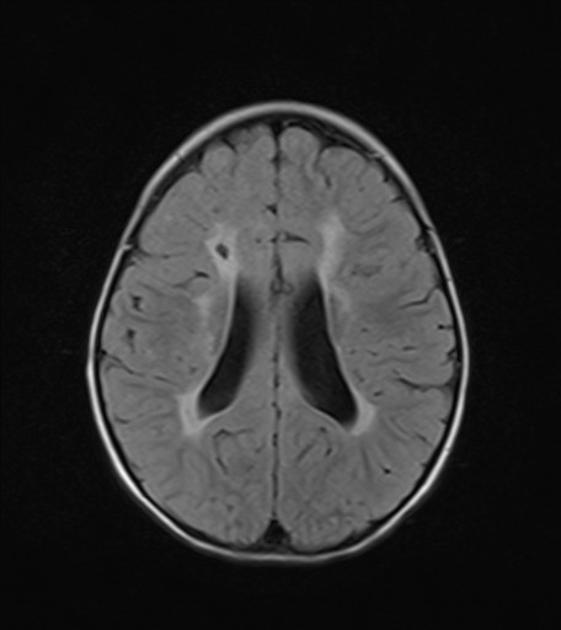
| MRI brain | Identify structural lesion |
| EEG | If seizures present |
| Genetic testing | If atypical features |
Neuroimaging Findings
Common MRI findings include:
- Periventricular leukomalacia
- Cortical malformations
- Brain atrophy
- Old infarction
Gross Motor Function Classification System (GMFCS)
This system classifies severity of CP.
| Level | Functional Ability |
|---|---|
| Level I | Walks independently |
| Level II | Walks with limitations |
| Level III | Walks with assistive device |
| Level IV | Limited self mobility |
| Level V | Wheelchair dependent |
Management of Cerebral Palsy
There is no cure, but multidisciplinary management improves function.
Multidisciplinary Treatment
| Therapy | Role |
|---|---|
| Physiotherapy | Improve mobility |
| Occupational therapy | Daily living skills |
| Speech therapy | Communication |
| Special education | Cognitive development |
Pharmacological Treatment
Used mainly for spasticity management.
| Drug | Mechanism |
|---|---|
| Baclofen | GABA agonist |
| Diazepam | Muscle relaxant |
| Tizanidine | Alpha-2 agonist |
| Botulinum toxin | Local spasticity control |
Surgical Management
Indicated in severe deformities.
Examples include:
- Tendon lengthening
- Hip reconstruction
- Selective dorsal rhizotomy
- Spinal surgery for scoliosis
Prevention Strategies
Important preventive measures include:
| Strategy | Benefit |
|---|---|
| Antenatal care | Prevent infections |
| Prevention of prematurity | Reduce PVL |
| Neonatal intensive care | Prevent brain injury |
| Early jaundice treatment | Prevent kernicterus |
Prognosis
Outcome depends on:
- Severity of brain injury
- Type of cerebral palsy
- Associated neurological deficits
- Access to rehabilitation
Many individuals with CP can live productive lives with appropriate therapy and support.
Clinical Pearls (High-Yield)
- Spastic diplegia → periventricular leukomalacia
- Dyskinetic CP → basal ganglia injury
- Ataxic CP → cerebellar damage
- Kernicterus → dyskinetic cerebral palsy
Conclusion
Cerebral palsy is a lifelong neurological disorder caused by early brain injury. Although the underlying brain damage is permanent, early diagnosis, multidisciplinary therapy, and supportive care can significantly improve functional outcomes and quality of life.