STANDARD TREATMENT PROTOCOL OF EMERGENCY HEALTH SERVICE PACKAGE
CONTENTS
 |
| STP BHS |
FOREWORD iii
ACKNOWLEDGEMENT V
ABBREVIATIONS X
BACKGROUND 1
Definition of Emergency Health Services 1
Rationale of the STP 2
Development Process of the STP 3
Utilization of the STP 3
Assumptions made for the implementation of the STP 4
How to use the STP 4
ABCDE Approach in the Emergency Room 7
Adult Basic Life Support 28
Paediatric Basic Life Support 29
Paediatric Cardiac Arrest Algorithm 30
Adult Cardiac Arrest Algorithm 31
Adult Tachycardia with a Pulse Algorithm 32
Adult Bradycardia Algorithm 33
Adult Post- Cardiac Arrest Care Algorithm 34
LIST OF EMERGENCY CONDITIONS 35
1. Respiratory Emergencies 37
2. Cardiac Emergencies 62
3. Neurological Emergencies 89
4. Gastrointestinal Emergencies 101
5. Genitourinary Emergencies 128
6. Gynaecology and Obstetrical Emergencies 135
7. Orthopedics and Trauma 152
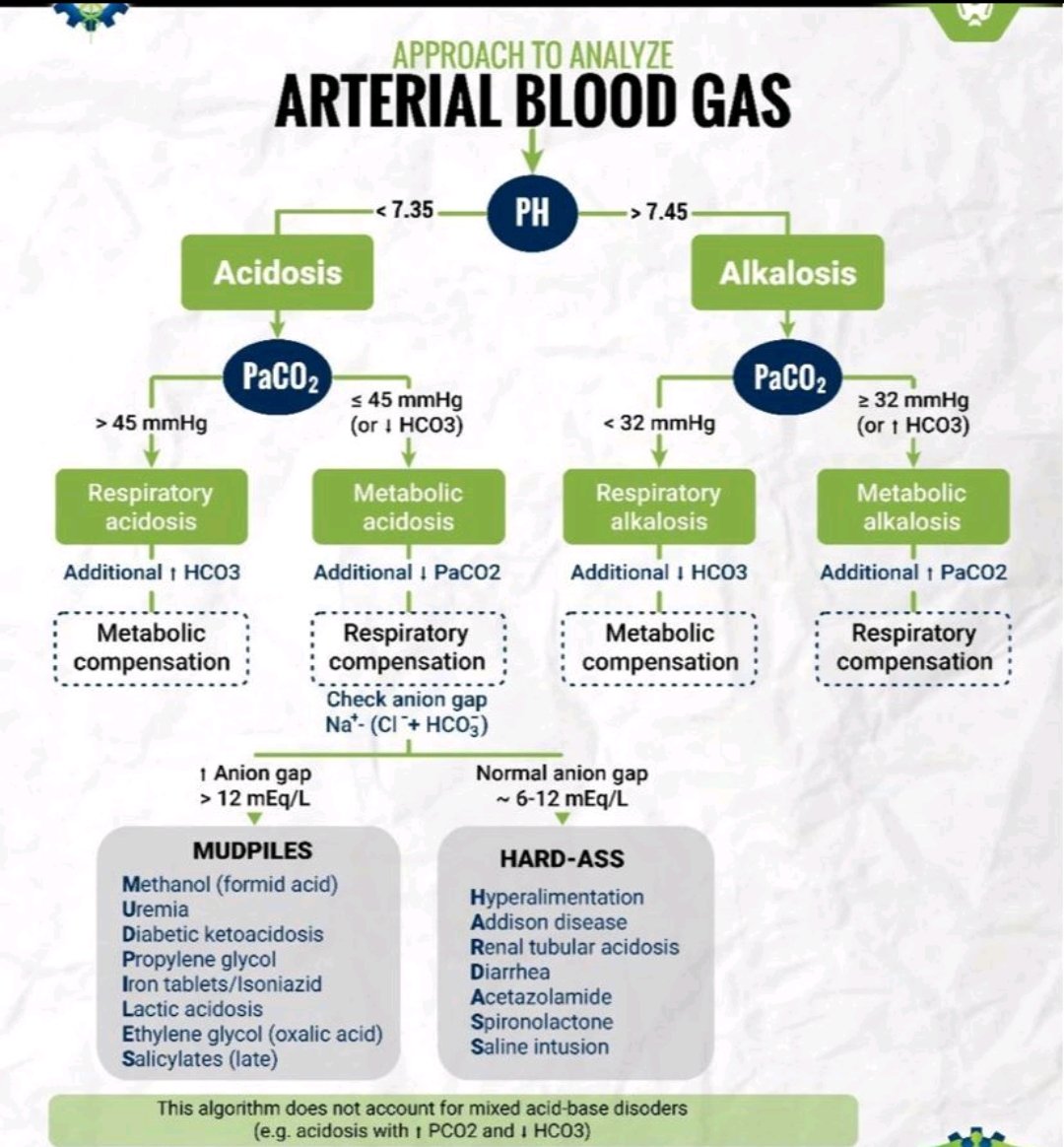
8. Metabolic Emergencies 168
9. Ocular Emergencies 179
10. ENT Emergencies 182
11. Burns 185
12. Mental Health Emergencies 191
13. Toxicological Emergencies 204
14. Snake bite, Animal bite, Insect bite 225
15. Pediatric Emergencies 234
16. Miscellaneous 244
STANDARD TREATMENT PROTOCOL OF EMERGENCY HEALTH SERVICE PACKAGE
viii
ANNEXES 253
ANNEX I: Schedule 2: Emergency Health Services 254
ANNEX II: List of Essential Medicines 257
Annex III: Patient Referral Form 270
ANNEX IV: Participants of Pre Planning/ Preliminary Consultative
Meeting with key government officials on STP of EHS 271
ANNEX V: Participants of Consultative TWG Meeting on STP of EHS 272
ANNEX VI: Participants of Consultative Meeting with Subjects/
Emergency Experts on STP of EHS 273
ANNEX VII: Participants of Consultative Meeting with Professional
Council and Association Members on STP of EHS 274
ANNEX VIII: Participants of High Level Consultative Meeting on STP of EHS 275
BIBLIOGRAPHY 277
STANDARD TREATMENT PROTOCOL OF EMERGENCY HEALTH SERVICE PACKAGE
ix
LIST OF FIGURES
Figure 1 Head tilt and chin lift 10
Figure 2 Head tilt and chin lift 10
Figure 3 Jaw thrust 11
Figure 4 Jaw thrust 11
Figure 5 Oropharyngeal airway (Guedel airway) 12
Figure 6 Nasopharyngeal airway 12
Figure 7 Bag and mask ventilation (One person technique) 13
Figure 8 Bag and mask ventilation (Two person technique) 13
Figure 9 LMA (Laryngeal mask airway) 14
Figure 10 Endotracheal tube 15
Figure 11 Cervical collar application 25
Figure 12 Cervical collar application 25
Figure 13 Log roll 27
Figure 14 Log roll 27
Figure 15 Acute anterior wall myocardial infarction 68
Figure 16 Acute inferior wall myocardial infarction 68
Figure 17 Atrial fibrillation with fast ventricular rate 76
Figure 18 Supraventricular tachycardia 78
Figure 19 Complete heart block