Introduction to Mechanical Ventilation
The mechanical ventilation is basically a replaement of assistance to the spontaneous ventilation/ breathing.
The concept of mechanical ventilation was first introduced by a scientist “Andreas Vesalius in 1555“
He said that : “an opening must be attempted in the trunk of the trachea, into which a tube of reed
or cane should be put; you will then blow into this, so that the lung may rise again . . .
and the heart becomes strong”
or cane should be put; you will then blow into this, so that the lung may rise again . . .
and the heart becomes strong”
This was the fundamental of development of mechanical ventilation and intubation but it took 400 years to apply this and actually use it in medical field.
Now a days mechanical ventilation has been the very vital part of medical sciece and has been used for many purposed in daily basis for saving millions of the lives worldwide.
Mecahnical ventilation and mechanicala ventilators have been used to save lives in emergency situations as well as in elective and emergency surgeries. They are the majr part of modern day ICU care.
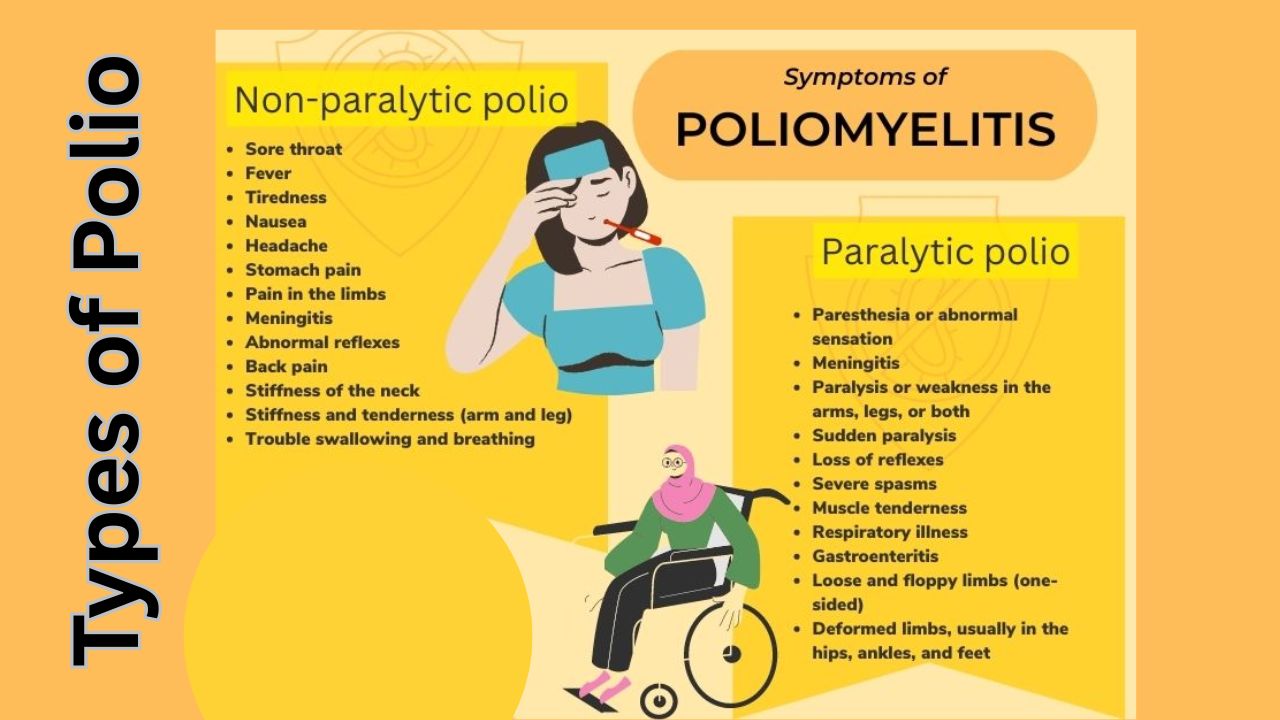
The first use of assisted ventilation (nt mechanical ventilations) was done in Europe during Polio outbreak (Read more about polio here).
Back then even human were used to a rtificailly ventilate the lung of sick people making them the human ventilators, and they even worked upto 8 hours a day and the medical schools were shut down for same purpose.
Later a company named “Ëmerson company” made a prototype positive pressure ventilator which was used in the Massachusetts General Hospital and it became instant succcess and started the era of Modern day intennsive care medicine.
What is Mechanical Ventilation? What happens when youre on a ventilator?
The basic concept of mechanical ventilation or positive pressure ventilation is to create a positive pressure the moves air/oxygen into the lungs. DUring breathing the pressure in our alveoli keeps on changing and during inspiration it becomes subatmospheric which drags air into the lungs and aveoli.
But if a person is not able to breathe by themselves in that condition positive pressure more than that of alveoli and lungs needs to be created by using artificial means and air or oxygen is pushed into the lungs.
 |
| A ventilator machine labelled different parts |
Mechanical Ventilation Definition
By undertanding above concept, mechanical ventilation can be difined as a process in which the lungs of a person who is not able to breath by oneself are inflated using external force, person or machine in order to push air into them and pull it back, in order to complete gaseous exchange, or for purpose of delivering medicine (in case of anesthesia or other critical care).
Understanding Mechanical Ventilation Settings
 |
| a bag-valve-mask |
In general there are two methods of positive pressure ventilation:
Volume controlled ventilation VC mode:
In this mode the initially the volume of air that is needed to be pushed into the ungs is selectd and ventilator selects the pressure needed to push that much volume into lungs by itself. Depending on that the rate of lung inflation, that if respiratory rate can be kept constant ot adjusted.
Pressure control ventilation PC mode:
In this mode the pressure at which the air/oxygen is pushed into lungs is preselected and duration and rate of lung inflation can be adjusted on the basis of need by the operator or doctor. by this desired tidal volume and sufficient oxygenation can be achieved.
The rate of lung inflation is initially high then is reduced so that presssure is same throughout(constant).
In other classification it can be classified as invasive and noninvasive ventilation:
Invasive ventilation
Invasive ventilation means ventilation with intubation in which a person a person has Endotrachea tube (ET Tube) placed in his trachea and through this air is supplied or his lungs are ventilated.
 |
| Endotracheal tube |
Non-inasive ventilation
Non invasive ventilation consists of CPAP and BiPAP. CPAP standa for continuous positive pressure ventilation and BiPAP mean bilevel positive pressure ventilation.
These both are achieved through a fitting mask kept covering nose and mouth of the patient.
Though these types of ventilation can also be achieved in invasive ventilation as well, unless not necessary a person is not intubated but CPAP / BiPAP mas is used for this purpose.
 |
| Volume control Vs Pressure control technique in mechanical ventilation |

Invasive Mechanical Ventilation: Benefits and Risks
Indication of mechanical ventilation
- Respiratory failure
- Hypoxemic respiratory failure : low oxygen saturation (sa02 or sp02)
- Hypercarbic respiratory failure: High carbondioxide content in blood (paCO2)
- Acute respiratory failure
- Ventilatory failure
- To reduce cerebral blood flow in case of raise ICP
- Prevent aspiration of gastric content or other foreign body
- Protect airway in seerely ill patient
- In intoxicated, poisoned patients
- To delever medicine and artificially breathe in case of general anesthesia
- Hemodynamic instability
- Heart attack
- Head, face and neck surgery
- Unstable or risky airway
- Cardiac arrest
- Encephalopathy
- Coma or deterirating GCS
 |
| Ventilated patient depiction drawing |
Befefits of mechanical ventilation:
- Proper and adequate oxygenation
- Accurate measurement of pressure and volumes
- Decreases work of breathing
- Improves gas exhange
- Reduces mortality
- Low failure rate than noninvasive ventilation
- Improves general pulmonary function
- Multiple modes available and settings can be changed according to need
- Stabilize and protects the airwat from collapse or obstruction
- Prevents aspiration
- Prevents atelectasis
- No airleaks
Risks associated with mechcanical ventilation:
- High pressure related lung injury : Barotrauma
- Volume trauma
- Oxygen toxicity
- Ventilator dependence
- Infection of airway
- Pneumonia, also called VAP : Ventilator associated pneumonia
- Mucus plug and lung collapse
- Airway trauma, mediastinal perforation
- Cuff presure injury to trachea and fistula formation, tracheal necrosis
- Hemodynamic collapse
- Tube malposition
- Electrolyte and aid base imbalance
- Mouth, teeth and lip trauma
- Infection of sinuses
- Muscle weakness and wasting and difficulty breathing after intubation later
- Position related complication
- Deep venous thrombosis and Pulmonary embolism (PE)
- Presure sores, ulcers
- Psychaitric problems
- Vocal cord injury and difficulty prducing speech
Mechanical Ventilation Systems: Types and Components
- Invasive ventilator with modern mamchine
- Bag-valve-mask ventilator (manual)
Though bag valve mask can also be connected to endotracheal tube.
 |
| ventilator |
Components of mechanical ventilator:
- Connector tube
- circuits
- t-piece
- HME filter
- monitor
- air and oxygen ports and supply
- ventilator machine
- power supply
- control knobs and butttons
 |
| ventilator parts |
Instruments needed for mechanical ventilation
- Ventilator machine
- Connecting tubes for oxygen deivery
- Endotracheal ET tube
- Syringes
- Stethoscope
- Direct laryngoscope
- Bag-Valve-Mask
- Suction machine
- Suction tube
- Source of oxygen
- Fixating tapes/dresings
- Medications for anesthesia and muscle relaxation
- Monitor for vitals monitering
- Trained manpower
Process of putting one into mechanical ventilator or starting mechnical ventilation
- The patient is decided for mechanical ventilation on basis of above mentioned criteria
- Patient is preoxygenatied
- Rapid sequence intubation is done using anesthetic agent and muscle relaxants
- Once intubation is done then patient is connected to ventilator machine with appropriate setttings
- The settings of the ventilator can be changed as need and patiend is intensively monitored
- Regularly check ABG to maintain arterial blood ga and electrolyte in limits
- Keep arterial blood pH 7.35-7.45
- Reularly check patient efforts, improvements, and treat the condition and cause of patiet’s need of intubation
- Follow strict precaution for infection prevention
- Prevent other complication

How does a ventilator work
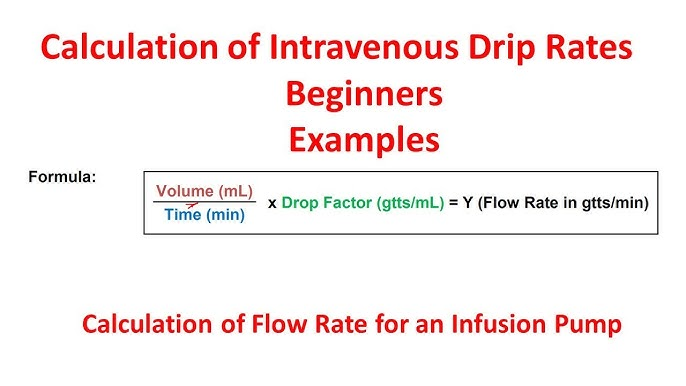
Method of ventilation-Lung Protective ventilatory strategy
- Set tidal volume to 6ml/kg
- calculate ideal body weight
- use VC and set initial tidal volume Vt to 8 ml/kg
- set RR to match baseline minute ventilation but not >35 bpm
- set PEEP to 5 cm of H2O
- reduce Vt by 1 ml/kg every 1-2 hr till its 6ml/kg
- adjust PEEP and FiO2 to maintain SpO2 88-95%
- Prevent plateau pressure exceedig 30 cm of water
- if plateau pressure .30 cm of water and Vt 6 ml/kg decrease vt 1 ml/kg until plateau pressure falls below 30 cm of water or Vt reached minimum of 4ml/kg
- use least possible concentreation of oxygent (fraction of inspired oxygen or FiO2) to maintain saturation more than 90%
- Adjust PEEP to maintain alveolar potency while preventing overdistention and closure reopening
- Ph goal to 7.30 to 7.45
- if pH 7.15-7.30 increase RR until ph >7.3, paco2 <25 or RR = 35
- if pH <7.15, increase RR=35. if still remains <7.15, increase Vt in 1ml/kg until pH>7.15
- if pH>7.45 decrease RR if possible
Read Normal ABG finding of a health person here:
Care during mechanical ventilation:
- Sedation and muscle relaxants or paralysis
- Analgesia
- Intensive monitoring
- Chest physiotherapy
- Suctioning and secretion clearing
- Nutrition
- Humidification
- Prevention of infection: common site of infections include lungs, urine, oral cavity, skin, and blood
- Mobilization
- Pressure prevention
- Thromboembolic prophylaxis
- Skincare
- Oralcare
- Eye care
- Other general care
 |
| ventilator in action |
Indication for discntinuation mechanical ventilation or indication of extubation
- Patients recovery
- Weaning
- Completion of indication
- Death
Technique of weaning:
SIMV wean
PS wean
T-piece trial
Some terminlogies related to mechanical ventilation:
Respiratory rate RR
Number of breathes (insiration and expiration = one breathe) per minute
Tidal volume Vt
The volume of air inhaled or exhaled in each breath / respiration by the person
Minute ventilation MV
Total volume inhald or exhaled by the person in a minute
FiO2
Fraction of the inhaled oxygen i.e percentage of oxygen in inhaled air
Peak pressure
The maximum pressure during inspiration generated by machine to push air into the lungs.
PEEP
Positive end expiratory pressure. It is the pressure at aveoli at the end of the expiration cycle before beginning of inspiration.
ACMV
Assist controlled mechanical ventilation
IMV
Intermittent mandatory ventilation
SIMV
Synchronized intermittent mandatory ventialtion
PSV
Pressure Support Ventilation
A/C, PCV
Assisted/Controlled, Pressure Controlled Ventilation (time cycled)
A/C, VCV
Assisted/Controlled, Volume Cycled Ventilation.
IRV
Inverse ratio ventilation
TCV
TIme controlled ventilation
ZEEP
Zero end expiratory pressure
NEEP
Negative end expiratry pressure
I:E ratio
Ratio of inspiratory time to expiratory time
SIMV + pressure support
Synchronized Intermittent Mandatory Ventilation with PEEP
CPAP
Continuous positive airway presssure
BiPAP
Bilevel positive aiway pressure
If you want to read more about above termnologie write us at mail@chaitanya.com.np
Some non-convetional ventilation strategies
- HFOV- high frequency oscillatory ventillation
- APRV- airway pressure release ventilation
- PLV- partial liquid ventilation
- ECMO- extracorporeal membrane oxygenation
- PAV- proportional assist ventilation
- NAV- neurally adjusted ventillatory-assist ventilation
- PAV-NAV : proportional assist ventilation-neurally adjusted ventillatory-assist ventilation
Read my friend’s blog at doctorhealthrx.com
Conclusion: Importance of Mechanical Ventilation
Mechanical ventilation is a medical technique that replaces or assists spontaneous breathing. The concept was first introduced in 1555 by Andreas Vesalius, but it took 400 years to develop mechanical ventilation into a medical practice.
Today, mechanical ventilation and ventilators are widely used for various purposes in medical care, including elective and emergency surgeries and emergency situations. There are two main methods of positive pressure ventilation, volume-controlled and pressure-controlled ventilation, which can be invasive or noninvasive.
Mechanical ventilation has many benefits, such as improving gas exchange, reducing the work of breathing, and improving general pulmonary function, but there are also risks, such as high pressure or lung damage. Overall, mechanical ventilation has been a crucial part of modern-day intensive care medicine and has saved millions of lives worldwide.