Please go through the pdf for tetanus prophylaxis guideline nepal 2023 below.
vaccine
Tetanus guideline
Appropriate tetanus prophylaxis should be administered as soon as possible following a wound but should be given even to patients who present late for medical attention. This is because the incubation period is quite variable; most cases occur within 8 days, but the incubation period can be as short as 3 days or as long as 21 days. For patients who have been vaccinated against tetanus previously but who are not up to date, there is likely to be little benefit in administering human tetanus immune globulin more than 1 week or so after the injury. However, for patients thought to be completely unvaccinated, human tetanus immune globulin should be given up to 21 days following the injury; Td or Tdap should be given concurrently to such patients
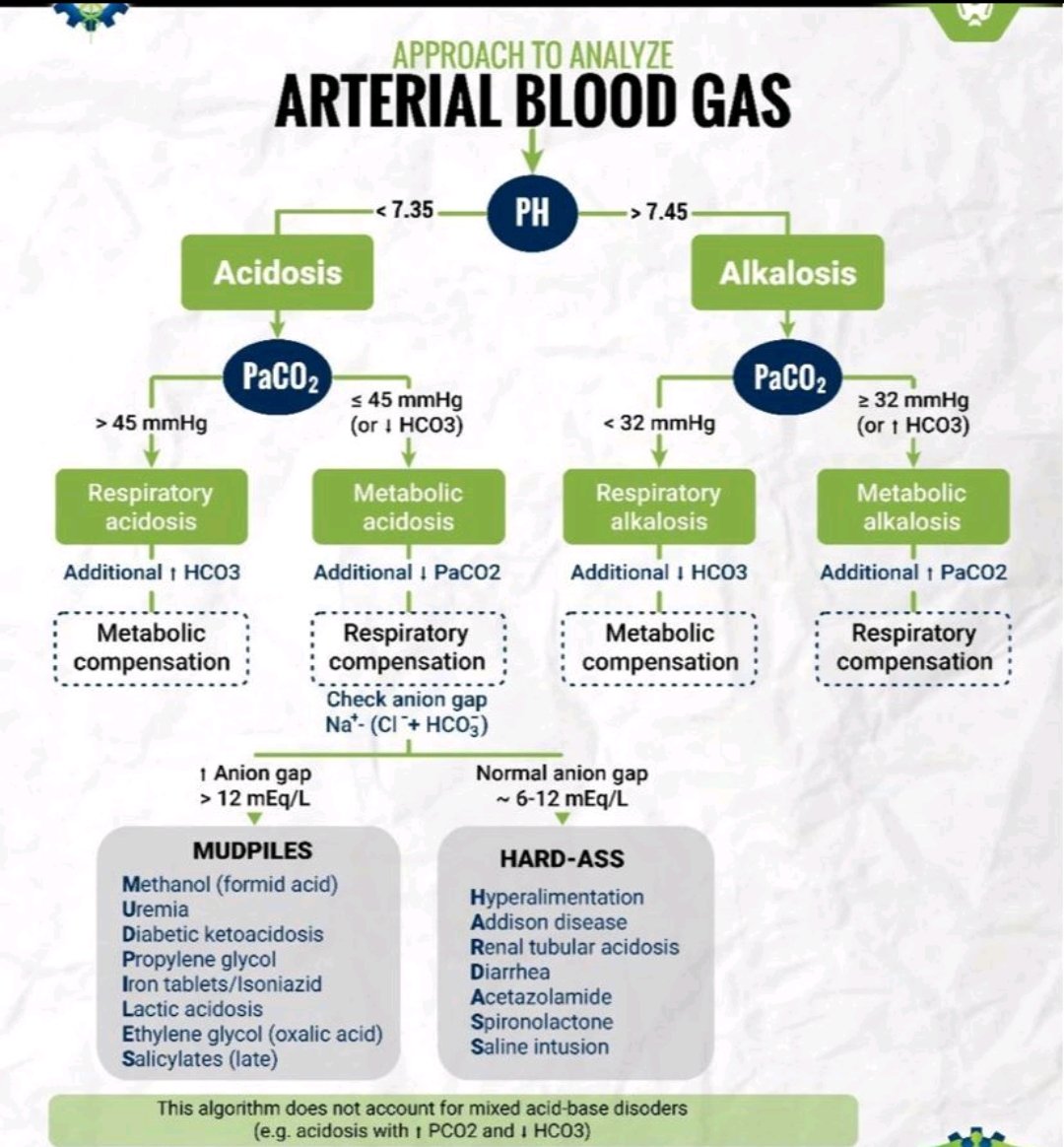
ABG stands for arterial blood gas. ABG is a common test done in case of critical care and severely ill patient to know the arterial bloog gas status of the patient along with various other parameters.