Definition:
A potentially fatal shift in fluids and electrolytes that occurs in malnourished patients when nutritional support (oral, enteral, or parenteral) is started too rapidly.
Pathophysiology:
Starvation → body switches to fat and protein metabolism, ↓ insulin, ↑ catabolism.
Refeeding with carbohydrate → ↑ insulin secretion → rapid cellular uptake of phosphate, potassium, magnesium.
Leads to hypophosphatemia (hallmark), hypokalemia, hypomagnesemia, thiamine deficiency, sodium/water retention.
Results in multi-system dysfunction.
Risk factors:
Severe malnutrition (BMI <16, >10% weight loss in 2–3 months).
Little or no intake >5–7 days.
Anorexia nervosa, cancer cachexia, chronic alcoholism, prolonged fasting, postoperative patients.
भिटामिन B3 ले फ्याटी लिभर रोगलाई नियन्त्रण गर्ने सम्भावना : नयाँ अनुसन्धानको उपलब्धि
Table of Contents (toc)
विश्व जनसंख्याको करिब ३० प्रतिशतलाई प्रभावित गर्ने मेटाबोलिक–एसोसिएटेड फ्याटी लिभर डिजिज (MASLD) हालसम्म प्रभावकारी लक्षित उपचारविहीन रोगका रूपमा परिचित थियो। तर, हालै गरिएको एक क्रान्तिकारी अनुसन्धानले यस रोगसँग सम्बन्धित प्रमुख आनुवंशिक कारण पत्ता लगाएको छ, र अझ चमत्कारिक कुरा त यो हो कि यसलाई नियन्त्रण गर्न सबैभन्दा प्रभावकारी औषधि भिटामिन B3 (नायसिन) भएको प्रमाणित भएको छ।
अनुसन्धानकर्ताहरूको खोज
दक्षिण कोरियाको युएनआइएसटी (UNIST) का प्रोफेसर जाङ ह्युन छोईको नेतृत्वमा, पुसान नेशनल युनिभर्सिटी (PNU) का प्रोफेसर ह्वायोङ युन र उल्सान युनिभर्सिटी अस्पताल (UUH) का प्रोफेसर न्युंग ह्वा पार्कको सहकार्यमा बनेको टोलीले पहिलो पटक विश्वस्तरमा MASLD को विकास र प्रगतिको क्रममा माइक्रोआरएनए–९३ (miR-93) को भूमिका स्पष्ट पारेका छन्।
miR-93 को प्रभाव
miR-93 लिभरका हेपाटोसाइट्स मा हुने विशेष RNA हो जसले केही लक्ष्य जीनहरूको अभिव्यक्तिलाई दवाउँछ। अनुसन्धानमा फ्याटी लिभर भएका बिरामी र जनावर दुवैमा miR-93 असामान्य रूपमा बढेको पाइएको छ।
यसले SIRT1 नामक जीनलाई रोक्दै लिभरको बोसो metabolism मा अवरोध गर्छ, जसका कारण लिभरमा बोसो जम्ने, सुजन बढ्ने र फाइब्रोसिस हुने अवस्था देखा पर्छ।
जनावरमा गरिएको परीक्षण
miR-93 लाई हटाइएका मुसामा लिभरमा बोसो जम्ने समस्या उल्लेख्य रूपमा घट्यो, साथै इन्सुलिन संवेदनशीलता र लिभर कार्यसम्बन्धी सूचकमा पनि सुधार आयो। उल्टै, miR-93 बढाइएका मुसामा लिभरको चयापचय अवस्था झन् बिग्रिएको देखियो।
भिटामिन B3 को चमत्कारिक प्रभाव
१५० वटा FDA–स्वीकृत औषधिहरूमध्ये, नायसिन (भिटामिन B3) ले miR-93 लाई सबैभन्दा प्रभावकारी रूपमा दबाउने देखियो। नायसिन सेवन गरिएका मुसामा miR-93 स्तर उल्लेख्य रूपमा घट्यो र SIRT1 सक्रिय भयो। यसले लिभरको बिग्रिएको बोसो चयापचयलाई पुनः सामान्य अवस्थामा ल्यायो।
अनुसन्धान टोलीका अनुसार,
“यस अध्ययनले MASLD को आणविक कारणलाई ठ्याक्कै स्पष्ट पारेको छ, साथै पहिले नै प्रयोगमा रहेको सुरक्षित भिटामिनलाई पुनःउपयोग गरेर उपचारमा नयाँ सम्भावना देखाएको छ।”
उपचारमा सम्भावना
नायसिन पहिले नै हाइपरलिपिडेमिया (रगतमा बोसो बढ्ने अवस्था) उपचारका लागि प्रयोग हुने सुरक्षित औषधि भएकाले, यो भविष्यमा MASLD का लागि संयुक्त उपचार (combination therapy) मा प्रयोग गर्न सकिने ठूलो सम्भावना देखिएको छ।
प्रकाशन र योगदान
यो अनुसन्धानलाई कोरिया नेशनल रिसर्च फाउन्डेशन (NRF) र कोरिया रिसर्च इन्स्टिच्युट अफ बायोसाइन्स एण्ड बायोटेक्नोलोजी (KRIBB) को सहयोग प्राप्त भएको थियो। अनुसन्धान नतिजा अन्तर्राष्ट्रिय ख्यातिप्राप्त जर्नल Metabolism: Clinical and Experimental मा प्रकाशित भएको छ।
अनुसन्धानमा UNIST का डा. यो हान ली र कियुन पार्क, उल्सान युनिभर्सिटी अस्पताल का प्रोफेसर जुनहो जुङ, र पुसान नेशनल युनिभर्सिटी की जिनयङ ली सह–प्रथम लेखकका रूपमा सहभागी भएका थिए।
References:
Yo Han Lee, Jinyoung Lee, Joonho Jeong, Kieun Park, Bukyung Baik, Yuseong Kwon, Kimyeong Kim, Keon Woo Khim, Haneul Ji, Ji Young Lee, Kwangho Kim, Ji Won Kim, Tam Dao, Misung Kim, Tae Young Lee, Yong Ryoul Yang, Haejin Yoon, Dongryeol Ryu, Seonghwan Hwang, Haeseung Lee, Dougu Nam, Won Kon Kim, Neung Hwa Park, Hwayoung Yun, Jang Hyun Choi. Hepatic miR-93 promotes the pathogenesis of metabolic dysfunction-associated steatotic liver disease by suppressing SIRT1. Metabolism, 2025; 169: 156266 DOI: 10.1016/j.metabol.2025.156266
Early-Onset Neonatal Sepsis refers to systemic infection occurring within the first 72 hours of life (some definitions extend up to 7 days in term neonates). It is a medical emergency characterized by a rapid progression from nonspecific signs to septic shock, multi-organ dysfunction, and death if not promptly treated.
The pathogenesis is primarily linked to vertical transmission of microorganisms from mother to infant, either intrauterine (transplacental hematogenous spread) or intrapartum (ascending infection from the genital tract during labor or delivery). Infection often develops after rupture of membranes, especially when prolonged (>18 hours), or in the setting of maternal fever, chorioamnionitis, or Group B Streptococcus (GBS) colonization.
Globally, EONNS remains a significant contributor to neonatal morbidity and mortality, particularly in low- and middle-income countries, where rates are higher due to limited access to intrapartum prophylaxis, delays in recognition, and suboptimal infection control during delivery. Mortality is highest in very low birth weight (VLBW) and preterm infants, where the immature immune system and compromised skin/mucosal barriers amplify vulnerability.
The microbiological profile varies by region. In high-income settings, GBS and Escherichia coli dominate, whereas in many developing countries, Gram-negative bacilli such as Klebsiella pneumoniae are increasingly prevalent. Importantly, EONNS often presents with respiratory distress, apnea, temperature instability, and lethargy, sometimes within minutes of birth.
Prompt diagnosis relies on high clinical suspicion, early blood cultures, and sepsis screening, followed by empiric antibiotic therapy (usually ampicillin plus gentamicin) while awaiting culture confirmation. Prevention strategies — especially maternal GBS screening and intrapartum antibiotic prophylaxis — have markedly reduced incidence in settings where implemented.
Late-Onset Neonatal Sepsis (LONNS)
Late-Onset Neonatal Sepsis refers to systemic infection occurring after 72 hours of life (or after 7 days in some term-based definitions) up to 28 days of age in term infants, and up to 44 weeks corrected gestational age in preterm infants. Unlike EONNS, its etiology is dominated by horizontal transmission of pathogens, often acquired in the hospital environment (nosocomial) or from community contacts after discharge.
LONNS frequently affects preterm and critically ill neonates in the neonatal intensive care unit (NICU), where prolonged hospitalization, mechanical ventilation, invasive procedures, and parenteral nutrition predispose to infection. Biofilm-forming organisms such as coagulase-negative staphylococci (CONS) exploit indwelling central venous catheters, while Gram-negative bacilli and fungi such as Candida spp. cause severe systemic illness, especially in extremely low birth weight (ELBW) infants.
Clinically, LONNS may have a more insidious onset than EONNS, often manifesting as apnea/bradycardia spells, feeding intolerance, abdominal distension, or subtle changes in behavior or perfusion. However, fulminant septic shock can occur, particularly in S. aureus, Klebsiella, or Pseudomonas infections. Meningitis is proportionally more common in LONNS due to delayed recognition and sustained bacteremia.
The microbial spectrum varies with hospital ecology, antibiotic use patterns, and infection control practices. In resource-limited settings, multidrug-resistant Gram-negative pathogens are a major concern, complicating empiric therapy. Common empiric regimens include vancomycin plus an aminoglycoside or ceftazidime/meropenem, tailored to local antibiograms.
Prevention of LONNS hinges on rigorous infection control measures: meticulous hand hygiene, bundle-based catheter care, minimizing unnecessary invasive devices, strict aseptic preparation of parenteral nutrition, and antimicrobial stewardship. While mortality in term infants is lower than in EONNS, LONNS remains a major cause of prolonged NICU stay, chronic lung disease, neurodevelopmental impairment, and death in preterm survivors.
Comparison Table – EONNS vs LONNS
Feature
Early-Onset Neonatal Sepsis (EONNS)
Late-Onset Neonatal Sepsis (LONNS)
Definition
Sepsis occurring within ≤72 hours of birth (some use ≤7 days in term, ≤72h in preterm)
Sepsis occurring after 72 hours (some use >7 days in term, >72h in preterm)
Primary Source of Infection
Vertical transmission from mother (intrauterine or intrapartum)
Horizontal transmission from environment, caregivers, or nosocomial sources
Mode of Transmission
Ascending infection after rupture of membranes, transplacental spread, exposure during passage through birth canal
Direct contact with infected personnel, contaminated equipment, invasive procedures
Common Risk Factors
– Maternal chorioamnionitis- Prolonged rupture of membranes (>18 h)- Maternal fever during labor- Preterm birth- GBS colonization- Low Apgar score
– Prolonged NICU stay- Indwelling central lines- Mechanical ventilation- Total parenteral nutrition (TPN)- Surgery- Cross-infection in NICU
Typical Pathogens
Term: Group B Streptococcus (GBS), E. coli, Listeria monocytogenes, Klebsiella, EnterococcusPreterm/NICU: Gram-negative bacilli (GNB), GBS
Gram-positive: Coagulase-negative staphylococci (CONS), S. aureusGram-negative: Klebsiella, E. coli, Pseudomonas, EnterobacterFungal: Candida spp. (esp. in VLBW on TPN)
Clinical Presentation
Rapid onset within first hours–days: respiratory distress, apnea, temperature instability, poor perfusion, hypotension, lethargy, seizures
More indolent onset: apnea/bradycardia spells, feeding intolerance, abdominal distension, lethargy, temperature instability, sepsis signs
CSF Findings (if meningitis)
Often presents concurrently with sepsis; E. coli, GBS common
More frequent with CONS, S. aureus, Candida; may follow prolonged bacteremia
Medical Officer – Lok Sewa Aayog (Public Service Commission)
Position: मेडिकल अधिकृत (Medical Officer) Grade: Eighth Level Service: Nepal Health Service – General Health Services Group
Exam Overview
The Eighth Level Open Competitive Examination for the Medical Officer position in the General Health Services Group is conducted in two phases:
First Phase – Written Examination
Full Marks: 200
Pass Marks: 40% in each paper
Language: Nepali, English, or both
Papers:
Paper I: General Health Services (MCQs) – 100 Marks
Paper II: General Health Services (Subjective) – 100 Marks
Second Phase – Group Test & Interview
Full Marks: 40 (10 for Group Discussion, 30 for Interview)
First Phase – Written Examination
Paper I: General Health Services (MCQs)
Marks: 100
Duration: 1 hr 15 min
Negative Marking: 20% deduction for each wrong answer; no deduction for unanswered questions
No calculators allowed
Paper II: General Health Services (Subjective)
Marks: 100
Duration: 3 hrs
Questions may be a single 10-mark question, multi-part questions, or short notes.
Separate answer booklets for each section must be used.
Second Phase – Group Test & Interview
Group Discussion
Marks: 10
Duration: 30 minutes
Format: Leaderless Group Discussion on a given topic
Includes turn-by-turn discussion and an individual presentation.
Evaluation Committee:
PSC Member – Chairperson
PSC Member – Member
Psychologist – Member
Subject Expert – Member
Interview
Marks: 30
Vacancy Fulfillment
Open Competition: 55% of total posts
Reserved Quotas (45%):
Women – 33%
Indigenous/Janajati – 27%
Madhesi – 22%
Dalit – 9%
Persons with Disabilities – 5%
Candidates from Backward Regions – 4%
Eligibility
Education
MBBS or equivalent from a recognized institution.
Age Limit
Minimum: 21 years
Maximum: 45 years (special provision under Health Service Group)
No age limit for permanent government employees.
Syllabus Summary
The syllabus covers General Health Services topics across multiple medical disciplines.
Both Paper I (MCQ) and Paper II (Subjective) will use the same syllabus.
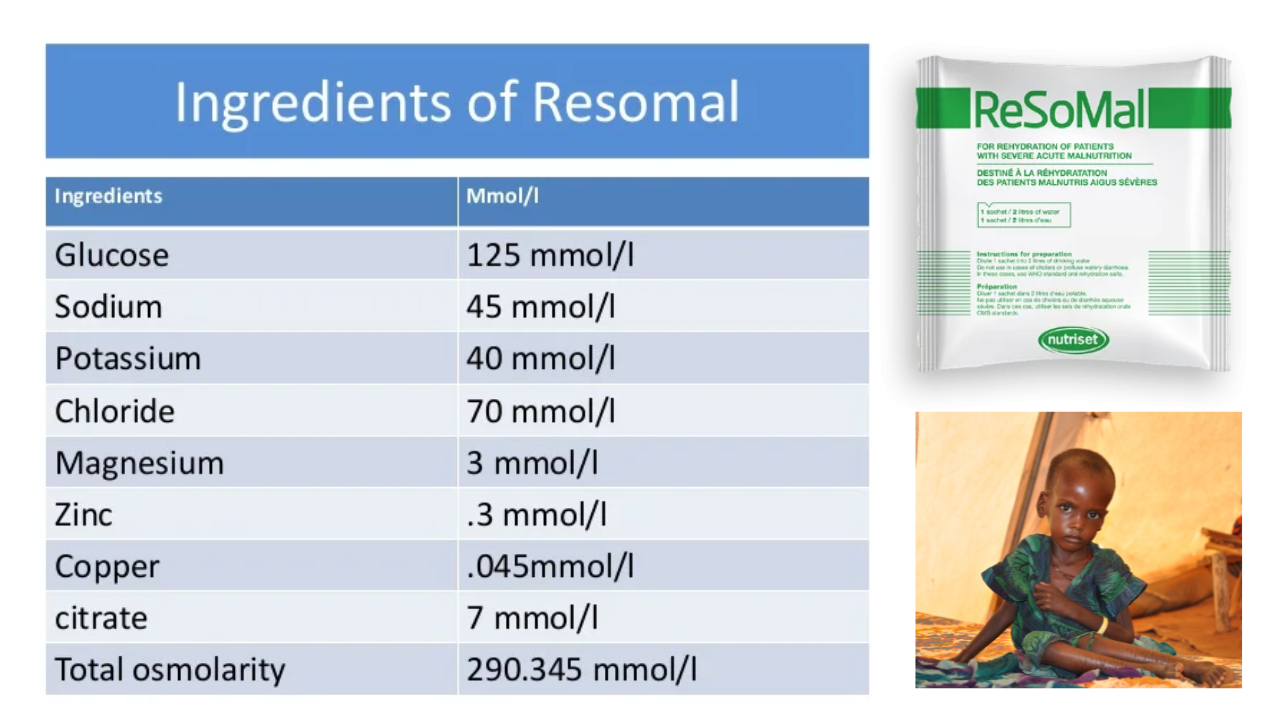
Severe acute malnutrition (SAM) complicates fluid and electrolyte balance, necessitating a specialized rehydration solution. ReSoMal—short for Rehydration Solution for Malnutrition—has lower sodium and higher potassium, plus added minerals like magnesium, zinc, and copper, making it safer for rehydration in SAM cases. It must be administered under medical supervision in therapeutic centers and is not for general use or for children with cholera.
Composition of WHO low osmolarity ORS
Component
Amount per Liter (g)
Concentration (mmol/L)
Osmolarity Contribution (mOsm/L)
Sodium chloride
2.6 g
Na⁺ 75 mmol Cl⁻ 65 mmol
75 + 65 = 140
Glucose anhydrous
13.5 g
75 mmol
75
Potassium chloride
1.5 g
K⁺ 20 mmol Cl⁻ 20 mmol
20 + 20 = 40
Trisodium citrate dihydrate
2.9 g
Citrate³⁻ 10 mmol Na⁺ 30 mmol
10 + 30 = 40
Total Osmolarity
21.5 g
–
245 mOsm/L
WHO low osmolarity ORS
Step-by-Step Guide: Preparing ReSoMal from Regular WHO ORS
Ingredients Needed (per 2 liters):
Boiled & cooled water: 2 liters
1 packet of WHO low-osmolar ORS (approx. 1-liter packet)
Sucrose (table sugar): 50 g
Concentrated electrolyte/mineral solution: 40 ml (optional; else use potassium chloride stock)
Preparation Instructions:
Mix the Water & ORS Packet Dissolve one WHO low-osmolar ORS packet in ~2 liters of clean, cooled water.
Add Sugar Stir in 50 g of sucrose (about 2 heaped tablespoons) to increase energy and glucose content.
Add Mineral Solution (if available)
Ideally, add 40 ml of electrolyte/mineral solution—it contains potassium, magnesium, zinc, copper, and other trace minerals.
If unavailable, substitute with 45 ml of potassium chloride (KCl) stock—prepared by dissolving 100 g KCl in 1 liter of water.
Administer with Caution
ReSoMal contains approximately 45 mmol sodium, 40 mmol potassium, and 3 mmol magnesium per liter.
Follow medical protocols: typical administration is around 5–10 ml per kg per hour, depending on the child’s condition.
Monitor closely for signs of overhydration—rapid weight gain, elevated respiratory or pulse rates, or peripheral edema—and pause treatment if they appear.
Why not use regular ORS?
Standard ORS has higher sodium and insufficient potassium for SAM, potentially risking fluid overload and undercorrected hypokalemia.
ReSoMal is tailored to reduce these risks—but it may still cause hyponatremia, so careful monitoring is essential.
It’s contraindicated in cases of cholera or profuse watery diarrhea, where standard WHO ORS is recommended instead.
Composition of ReSoMal (WHO formulation for severe malnutrition)
Component
Amount per Liter (g)
Concentration (mmol/L)
Osmolarity Contribution (mOsm/L)
Sodium chloride
1.5 g
Na⁺ 45 mmol Cl⁻ 37 mmol
45 + 37 = 82
Glucose anhydrous
25 g
139 mmol
139
Potassium chloride
3.5 g
K⁺ 40 mmol Cl⁻ 40 mmol
40 + 40 = 80
Magnesium chloride
0.3 g
Mg²⁺ 3 mmol Cl⁻ 6 mmol
3 + 6 = 9
Zinc acetate
0.03 g
Zn²⁺ 0.3 mmol
0.3
Copper sulphate
0.003 g
Cu²⁺ 0.05 mmol
0.05
Trisodium citrate dihydrate
0.6 g
Citrate³⁻ 7 mmol Na⁺ 21 mmol
7 + 21 = 28
Total Osmolarity
–
–
300 mOsm/L
WHO recommended ReSoMal
Summary Table
Item
Details
Purpose
Rehydration for children with severe acute malnutrition (SAM)
Base Ingredients
WHO ORS packet, water, sugar, optional electrolyte solution
Substitution Option
Use KCl stock if mineral blend isn’t available
Administration
Slow and monitored—5-10 ml/kg/hour or as per protocol
Key Warnings
Not for cholera; risk of overhydration and hyponatremia
Summary and Conclusion
ReSoMal is a life-saving adaptation of ORS for malnourished children—but it’s delicate medicine. Always follow WHO protocols and local medical guidelines, and never administer without proper training and monitoring.
The image provided shows a newborn child with a characteristic position of the right upper limb.
The arm appears to be adducted and internally rotated at the shoulder, with the forearm extended and pronated. This posture is suggestive of a birth-related brachial plexus injury.
Considering the typical clinical presentations of the options provided:
Klumpke’s paralysis:
This affects the lower roots of the brachial plexus (C8-T1), leading to weakness or paralysis of the forearm and hand muscles, often presenting with a claw hand deformity. It doesn’t match the position seen in the image.
Erb’s palsy:
This is an injury to the upper roots of the brachial plexus (C5-C6, and sometimes C7), which typically presents with the arm hanging by the side and rotated medially, with the forearm extended and pronated – a position known as “waiter’s tip.”
This condition closely matches the posture seen in the image.
Long thoracic nerve palsy:
This would primarily affect the serratus anterior muscle, leading to “winged scapula” but wouldn’t cause the arm positioning depicted in the image.
Thoracic outlet syndrome:
This is highly unlikely in a newborn, as it generally results from compression of the brachial plexus or subclavian vessels in the area between the base of the neck and the armpit, seen in older patients.
Given the posture of the arm and the typical presentation of these conditions, Erb’s palsy
(B) is the most likely diagnosis.
This condition is commonly associated with birth trauma, particularly in deliveries involving shoulder dystocia
Understanding Hormonal Disorders and Electrolyte Imbalances
Certain endocrine disorders can significantly alter the balance of sodium (Na⁺) and potassium (K⁺) in the body, leading to characteristic clinical presentations. Here, we examine three important conditions—Conn’s disease, Addison’s disease, and Cushing syndrome—and their effects on electrolyte regulation.
Q. Which of the following conditions is most likely to present with increased sodium (↑ Na⁺) and decreased potassium (↓ K⁺)?
d) All of the aboveConn’s Disease (Primary Hyperaldosteronism)
Conn’s disease is caused by excessive secretion of aldosterone, a hormone that promotes sodium reabsorption and potassium excretion in the kidneys. This hormonal excess leads to:
↑ Na⁺ (hypernatremia) due to sodium retention
↓ K⁺ (hypokalemia) due to increased potassium loss
Resulting clinical features: hypertension and muscle weakness from hypokalemia
Because both increased sodium and decreased potassium occur, Conn’s disease perfectly fits the profile for this electrolyte change.
conn disease
Addison’s Disease (Primary Adrenal Insufficiency)
Addison’s disease is characterized by insufficient production of both aldosterone and cortisol. This deficiency results in:
↓ Na⁺ (hyponatremia) due to reduced sodium reabsorption
↑ K⁺ (hyperkalemia) due to impaired potassium excretion
Associated symptoms: low blood pressure, fatigue, and skin hyperpigmentation
Since sodium is low and potassium is high, Addison’s disease does not match the criteria for increased Na⁺ and decreased K⁺.
adrenal insufficiency
Cushing Syndrome (Excess Cortisol)
Cushing syndrome is caused by prolonged exposure to elevated cortisol levels. While cortisol primarily affects glucose metabolism, it can have mineralocorticoid-like effects in certain situations, leading to:
Mild sodium retention
Hypertension
Potassium levels typically remain normal, unless there is marked mineralocorticoid activity (as seen in ectopic ACTH production)
Cushing Syndrome (Excess Cortisol)
Thus, Cushing syndrome generally does not cause the significant hypokalemia seen in Conn’s disease.
Summary: Who Fits the Criteria?
The combination of increased sodium (↑ Na⁺) and decreased potassium (↓ K⁺) is a hallmark of Conn’s disease. Addison’s disease produces the opposite electrolyte pattern, and Cushing syndrome rarely causes a significant drop in potassium unless in special cases.
Correct answer:b) Conn’s disease
Condition
Hormone Change
Sodium (Na⁺)
Potassium (K⁺)
Blood Pressure
Key Notes
Conn’s Disease (Primary Hyperaldosteronism)
↑ Aldosterone
↑ (Retention)
↓ (Excretion)
↑ (Hypertension)
Classic ↑ Na⁺ + ↓ K⁺ pattern
Addison’s Disease (Primary Adrenal Insufficiency)
↓ Aldosterone & ↓ Cortisol
↓ (Loss)
↑ (Retention)
↓ (Hypotension)
Opposite pattern to Conn’s
Cushing Syndrome (Excess Cortisol)
↑ Cortisol
↑ (Mild retention)
Usually Normal (↓ only if excess mineralocorticoid effect)





















")



