Meningitis, encephalitis and stroke for medical students preparation slide:
Table of Contents (toc)
Introduction and definition of meningitis:
Meningitis is the inflammation of the CSF and the meninges. If the
infection spreads into the brain it is termed meningoencephalitis. Usually is caused by an infection, but chemical meningitis also may occur
in response to a nonbacterial irritants introduced into the subarachnoid
space.
Types of meningitis:
Infectious meningitis can be broadly divided into:
NEPAL DEMOGRAPHIC AND HEALTH SURVEY (NDHS) 2022 KEY INDICATORS
Table of Contents(toc)
Introduction: latest ndhs report of nepal
The 2022 Nepal Demographic and Health Survey (2022 NDHS) was implemented by New ERA under the aegis of the Ministry of Health and Population of Nepal. The funding for the NDHS was provided by the United States Agency for International Development (USAID). ICF provided technical assistance through The DHS Program, a USAID-funded project providing support and technical assistance in the implementation of population and health surveys in countries worldwide. It replaces ndhs 2016 which is past report.
ndhs 2022 report
NDHS full form
Nepal demographic and household survey.
The contents of this report are the sole responsibility of the Ministry of Health and Population, New ERA, and
ICF.
This Key Indicators Report presents a first look at selected findings from the 2022 NDHS. A
comprehensive analysis of the data will be presented in a final report in 2023.
Objectives NDHS survey 2022
The primary objective of the 2022 NDHS is to present up-to-date estimates of basic demographic and
health indicators. The NDHS provides a comprehensive overview of population, maternal, and child health
issues in Nepal. Specifically, the 2022 NDHS collected information on fertility levels, marriage, fertility
preferences, awareness and use of family planning methods, breastfeeding practices, nutrition, maternal
and child health, childhood mortality, awareness and behavior regarding HIV and other sexually
accident and injury, disability, food insecurity, and other health-related issues such as smoking, knowledge
of tuberculosis, and prevalence of hypertension.
The information collected through the 2022 NDHS is intended to assist policymakers and program
managers in designing and evaluating programs and strategies for improving the health of Nepal’s
population. The 2022 NDHS also provides indicators relevant to the Nepal Health Sector Strategy 2016–
22, the next health sector strategic plan under development, and the Sustainable Development Goals
(SDGs) for Nepal.
SURVEY IMPLEMENTATION
SAMPLE DESIGN
The sampling frame used for the 2022 NDHS is an updated version of the frame of the Nepal Population and Housing Census (NPHC) conducted in 2011, provided by the Central Bureau of Statistics. The smallest administrative unit in Nepal is the sub-ward.
The census frame includes a complete list of Nepal’s 36,020 sub-wards. Each sub-ward has a residence type (urban or rural) and a measure of size is the number of households.
In September 2015, Nepal’s Constituent Assembly declared changes in the administrative units and a re- classification of urban and rural areas in the country. Nepal is divided into seven provinces: Province 1, Madhesh Province, Bagmati Province, Gandaki Province, Lumbini Province, Karnali Province, and Sudurpashchim Province.
Each province is divided into districts, districts into municipalities, municipalities into wards, and wards into sub-wards. Nepal has 77 districts, which include a total of 753 (local level) municipalities. Of the municipalities, 293 are urban and 460 are rural. Originally, the 2011 NPHC included 58 urban municipalities. This number increased to 217 by 2015.
On March 10, 2017, structural changes were made in the classification system for urban (Nagarpalika) and rural (Gaonpalika) locations. Nepal currently has 293 Nagarpalika, with 65% of the population living in these urban areas. The 2022 NDHS used this updated urban-rural classification system.
The 2022 NDHS sample is a stratified sample selected in two stages. Stratification was achieved by dividing each of the seven provinces into urban and rural areas which together formed the sampling stratum for that province.
A total of 14 sampling strata were created in this way. Implicit stratification with proportional allocation was achieved at each of the lower administrative levels by sorting the sampling frame within each
sampling stratum before sample selection, according to administrative units in the different levels, and by
using a probability-proportional-to-size selection at the first stage of sampling. In the first stage of
sampling, 476 primary sampling units (PSUs) were selected with probability proportional to the PSU size and with independent selection in each sampling stratum within the sample allocation.
Among the 476 PSUs, 248 were from urban areas and 228 were from rural areas. A household listing operation was carried out in all the selected PSUs before the main survey. The resulting list of households served as the sampling frame for the selection of sample households in the second stage.
Thirty households were selected from each cluster, for a total sample size of 14,280 households. Of these, 7,440 households were in urban areas, and 6,840 households were in the rural areas. Some of the selected sub-wards were found to be overly large during the household listing operation. Selected sub-wards with an estimated number of households greater than 300 were segmented.
Only one segment was selected for the survey with probability proportional to the segment size. Global positioning system (GPS) data was collected at the household level during the household listing and the individual interviews.
Four questionnaires were used for the 2022 NDHS: the Household Questionnaire, the Woman’s
Questionnaire, the Man’s Questionnaire, and the Biomarker Questionnaire. The questionnaires, based on
The DHS Program’s standard Demographic and Health Survey (DHS-8) questionnaires, were adapted to reflect the population and health issues relevant to Nepal. In addition, a self-administered Fieldworker Questionnaire collected information about the survey’s fieldworkers.
Input was solicited from various stakeholders representing government ministries and agencies, nongovernmental organizations, and international donors. The survey protocol was reviewed by the Nepal Health Research Council and the ICF Institutional Review Board. The 2022 NDHS required written consent from the household head to carry out the interviews and to test for anemia.
Similarly, written consent/assent was required from individuals for anemia testing and from parents/guardians for children age 6–59 months.
After all questionnaires were finalized in English, they were translated into Nepali, Maithili, and Bhojpuri languages. The Household, Woman’s, and Man’s Questionnaires were programmed into tablet computers to facilitate computer-assisted personal interviewing (CAPI) for data collection purposes, with the capability to choose any of the three languages for each questionnaire. The Biomarker Questionnaire was completed on paper during the data collection and then entered in the CAPI system.
Woman’s questionnaire NDHS 2022
The Woman’s Questionnaire was used to collect information from all women age 15–49. These women
were asked questions on the following topics:
Background characteristics (including age, education, and media exposure)
Pregnancy history and child mortality
Knowledge, use, and source of family planning methods
Fertility preferences (including desire for more children, ideal number of children)
Antenatal, delivery, and postnatal care
Vaccinations and childhood illnesses
Breastfeeding and infant feeding practices
Women’s work and husbands’ background characteristics
Knowledge, awareness, and behavior regarding HIV and other sexually transmitted infections (STIs)
Fistula
Mental health
Domestic violence
Knowledge, attitudes, and behavior related to other health issues (for example, cancer, smoking, tuberculosis, and COVID-19)
KEY findings of NDHS 2022 report
RESPONSE RATES
Table 1 shows the results of the household and individual interviews, and response rates, according to
residence, for the 2022 NDHS. A total of 14,243 households were selected for the 2022 NDHS sample, of which 13,833 were found to be occupied. Of the occupied households, 13,786 were successfully
interviewed, yielding a response rate of 99.7%.
In the interviewed households, 15,238 women age 15–49 were identified as eligible for individual interview. Interviews were completed with 14,845 women, yielding a response rate of 97%. In the subsample of households selected for the men’s survey, 5,185 men age 15–49 were identified as eligible for individual interview and 4,913 were successfully interviewed, yielding a response rate of 95%.
FERTILITY repot on NDHS 2022
Under SDG 3.7.1 (b) the government of Nepal targets achieving a total fertility rate of 2.1 births per
woman by 2030 (National Planning Commission, 2020). Table 3 shows the total fertility rate (TFR) and
the age-specific fertility rates (ASFRs) among women by 5-year age groups for the 3-year period
preceding the survey.
Total fertility rate
The average number of children a woman would have by the end of her
childbearing years if she bore children at the current age-specific fertility rates.
Age-specific fertility rates are calculated for the 3 years before the survey,
based on detailed pregnancy histories provided by women.
Sample: Women age 15–49
▪ If fertility were to remain constant at current levels, a woman in Nepal would bear an average of 2.1
children in her lifetime.
▪ Fertility is low among adolescents (71 births per 1,000 women age 15–19), peaks at 160 births per
1,000 among women age 20–24, and then deceases thereafter.
TEENAGE FERTILITY ndhs 2022 nepal
Teenage pregnancy
Percentage of women age 15–19 who have ever been pregnant.
Sample: Women age 15–19
Table 4 shows the percentage of women age 15–19 who have ever been pregnant at the time of the survey,
according to background characteristics.
▪ Overall, 14% of women age 15–19 have ever been pregnant, including 10% who have had a live birth,
2% who have had a pregnancy loss, and 4% who are currently pregnant.
The percentage of women age 15–19 who have ever been pregnant rises with age, from 1% at age 15
to 32% by age 19.
▪ Teenage pregnancy is highest in Karnali Province (21%), followed by Madhesh Province (20%), and
lowest in Bagmati Province (8%).
▪ Women age 15–19 with no education (33%) are more likely to start childbearing earlier than those
with at least some secondary education (8%).
FERTILITY PREFERENCES
Desire for another child
Women were asked whether they wanted more children and, if so, how long
they would prefer to wait before the birth of the next child. Women who are
sterilized are assumed not to want any more children.
Sample: Currently married women age 15–49
Information on fertility preferences is used to assess the potential demand for family planning services for
the purposes of spacing or limiting future childbearing. Table 5 shows fertility preferences among
currently married women age 15–49 by number of living children.
▪ Ten percent (10%) of women want another child soon (within the next 2 years), 13% want to have
another child later (in 2 or more years), and 1% want another child but have not decided when.
▪ Fifty-three percent (53%) of women want no more children, 17% are sterilized, and 3% stated that
they are infecund.
▪ The percentage of women who want another child soon decreases from 59% among those with no
living children to 2% or less among those with three or more children. In general, the more children a
woman has, the higher the likelihood that she does not want another child or is sterilized.
FAMILY PLANNING ndhs 2022 nepal
Contraceptive use
Contraceptive prevalence
Percentage of women who use any contraceptive method.
Sample: Currently married women age 15–49
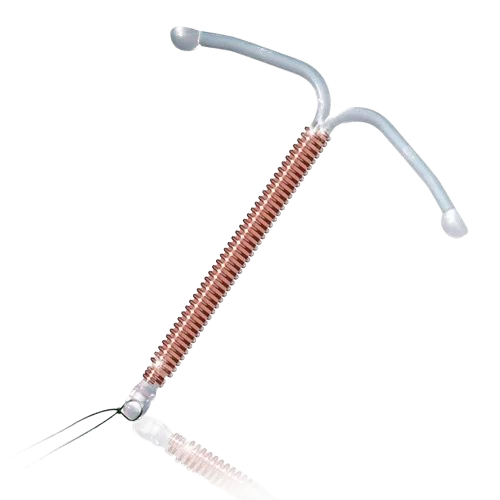
Modern methods
Include male and female sterilization, injectables, intrauterine contraceptive
device (IUCD), contraceptive pill, implants, male condoms, emergency
contraception, the standard days method, and lactational amenorrhea method.
The government of Nepal’s target under SDG 3.7.1 (a) includes specific targets for use of modern methods
of contraception by women of reproductive age (15–49). The targets are 53% by 2022 and 60% by 2030
(Ministry of Health and Population 2022). Table 6 shows current levels of contraceptive use among
currently married women age 15–49.
▪ Fifty-seven (57%) of currently married women are using a method of contraception; 43% are using a
modern method, and 15% are using a traditional method.
▪ The most popular modern methods used are female sterilization (13%), injectables (9%), and implants
(6%).
▪ Withdrawal is by far the most common traditional method used; 13% of currently married women use
this method compared with 2% who use the rhythm method.
Trends: Use of any family planning method among currently married women rose from 29% in 1996 to
57% in 2022. Over the same period, use of modern methods of contraception increased from 26% in 1996
to 44% in 2006. It has held steady at 43% from 2011 through 2022
need for family planning NDHS 2022
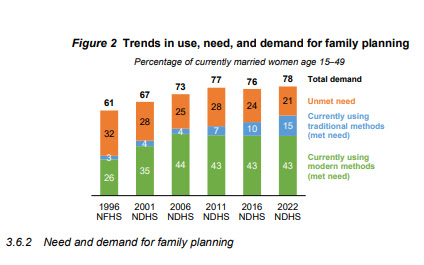
Need and demand for family planning
Table 7 presents data on unmet need, met need, and total demand for family planning among currently
married women. These indicators help evaluate the extent to which family planning programs in Nepal are
meeting the demand for services. The government of Nepal’s target for SDG 3.7.1, is that 74% of all
women age 15–49 have a met need for family planning with modern methods by 2022 and 80% by 2030
(National Planning Commission 2020).
Twenty-one percent (21%) of currently married women in Nepal have an unmet need for family
planning services. Fifty-seven percent (57%) of currently married women are currently using a
contraceptive method. Therefore, 78% of currently married women have a demand for family
planning. Thus, if all married women who said they want to space or limit their children were to use
family planning methods, the contraceptive prevalence rate would increase from 57% to 78%.
▪ The total demand for family planning that is satisfied is 73%; 55% of the total demand is satisfied by
modern methods.
EARLY CHILDHOOD MORTALITY ndhs 2022 nepal
Neonatal mortality: The probability of dying within the first month of life.
Postneonatal mortality: The probability of dying between the first month of
life and the first birthday (computed as the difference between infant and
neonatal mortality).
Infant mortality: The probability of dying between birth and the first birthday.
Child mortality: The probability of dying between the first and fifth birthday.
Under-5 mortality: The probability of dying between birth and the fifth
birthday.
The government of Nepal’s target for SDG 3.2.1, is to reduce the under-five mortality rate to 27 deaths per
1,000 live births by 2022 and to 20 deaths per 1,000 live births by 2030. Similarly, the government’s target
for SDG 3.2.2, is to reduce the neonatal mortality rate to 16 deaths per 1,000 live births by 2022 and to 12
deaths per 1,000 live births by 2030 (National Planning Commission, 2020).
Table 8 presents estimates of early childhood mortality rates for three successive 5-year periods prior to
the 2022 NDHS. The rates are estimated directly from the information collected as part of a retrospective
pregnancy history, in which female respondents list all of the children to whom they have given birth,
along with each child’s date of birth, survivorship status, and current age or age at death.
▪ During the 5 years immediately preceding the survey, the overall under-5 mortality rate was 33 deaths
per 1,000 live births.
▪ The infant mortality rate was 28 deaths per 1,000 live births. The child mortality rate was 5 deaths per
1,000 children surviving to age 12 months.
▪ The neonatal mortality rate was 21 deaths per 1,000 live births, during the 5 years immediately
preceding the survey.
▪ Eighty-five percent (85%) of all deaths among children under age 5 in Nepal take place before a
child’s first birthday, with 64% occurring during the first month of life.
MATERNAL CARE
Proper care during pregnancy and delivery is important for the health of both the mother and the baby.
Table 9 presents key indicators related to maternal care.
3.8.1 Antenatal care
Antenatal care (ANC) from a skilled provider
Pregnancy care received from skilled providers, such as doctors, nurses, and
auxiliary nurse midwives.
Sample: Women age 15–49 who had a live birth or stillbirth in the 2 years
preceding the survey
Antenatal care (ANC) from a skilled provider is important to monitor pregnancy and reduce morbidity and
mortality risks for the mother and child during pregnancy, at delivery, and during the postnatal period.
▪ Ninety-four percent (94%) of women reported receiving antenatal care from a skilled provider for their
most recent live birth or stillbirth in the 2-year period preceding the survey.
▪ Four in five women (81%) had at least four ANC visits for their most recent live birth.
▪ Overall, 96% of women took iron-containing supplements during their most recent pregnancy.
Trends: The percentage of women who received antenatal care from skilled provider for their most recent
live birth in the 2 years preceding the survey increased from 25% in 1996 to 94% in 2022. Similarly, those
who made four or more ANC visits increased from 9% in 1996 to 81% in 2022.
Tetanus toxoid
Protection against neonatal tetanus
The number of tetanus toxoid injections needed to protect a baby from
neonatal tetanus depends on the mother’s vaccinations. A birth is protected
against neonatal tetanus if the mother has received any of the following:
▪ Two tetanus toxoid injections during the pregnancy
▪ Two or more injections, the last one within 3 years of the birth
▪ Three or more injections, the last one within 5 years of the birth
▪ Four or more injections, the last one within 10 years of the birth
▪ Five or more injections at any time prior to the birth
Sample: Women age 15-49 with a live birth in the 2 years preceding the
survey
Delivery care
Institutional deliveries
Deliveries that occur in a health facility.
Sample: All live births and/or stillbirths in the 2 years preceding the survey
Skilled assistance during delivery
Births delivered with the assistance of a doctor, nurse, or midwife.
Sample: All live births and/or stillbirths in the 2 years preceding the survey
Access to proper medical attention and hygienic conditions during delivery can reduce the risk of
complications and infections that may lead to death or serious illness for the mother and/or baby (Van
Lerberghe and De Brouwere 2001; WHO 2006a). The government of Nepal’s target for SDG 3.1.2, is that
73% of births are delivered with assistance from skilled provider by 2022 and achieve 90% by 2030
(National Planning Commission 2020).
▪ Overall, 79% of live births and still births in the 2 years preceding the survey were delivered in health
facilities.
▪ Four in five (80%) live births and stillbirths were delivered by skilled providers.
Trends: The percentage of live births that are assisted by a skilled provider has increased markedly, from
10% in 1996 to 80% in 2022)
Postnatal care for the mother ndhs 2022 nepal
A large proportion of maternal and neonatal deaths occur during the first 48 hours after delivery. Thus,
prompt postnatal care (PNC) for both the mother and the child is important to treat any complications
arising from the delivery, as well as to provide the mother with important information on how to care for
herself and her child. Safe motherhood programs recommend that all women receive a health check during
the first 2 days after birth.
▪ Overall, 70% of women with a live birth or stillbirth in the 2 years preceding the survey received a
postnatal check within the 2 days after delivery.
▪ Among women with a live birth, women in the lowest wealth quintile are less likely to receive
postnatal check within 2 days after delivery than women in the highest wealth quintile (56% versus
87%).
maternal mortality rate in nepal ndhs 2016
check text above
VACCINATION COVERAGE
Universal immunization of children against common vaccine-preventable diseases is crucial to reducing
infant and child morbidity and mortality. In Nepal, routine childhood vaccines include bacillus Calmette-
Top 20 Signs and symptoms of Pregnancy in early and mid phase Explained
Pregnant or Not pregnant
Table of Contents (toc)
Introduction
Pregnancy has been nature’s way of maintaining homeostasis. It’s considered physiological process to maintain life and continue life on earth.
All the mammals get pregnant in order to give birth to their offspring.
As being mammal same applies for the human beings as well.
It can be very difficult to diagnose pregnancy in the early phase and sometimes pregnancy can be confused with other medical illnesses as well and the patient may seek treatment for their symptoms in multiple clinical setting.
Hence it is necessary for us to ask the last menstrual period to the patient and suspect the possible menstrual cession due to pregnancy.
It’s also necessary for us to diagnosed pregnancy on the basis of symptoms and science to avoid the territogenic drugs in case of early pregnancy particularly because territory drugs have effect on early pregnancy more than on later pregnancy.
List of teratogenic drug the we commonly prescribe is listed separately on this article.
Now let’s move to common signs and symptoms of pregnancy that we need to ask and note down and also check during clinical examination to diagnose pregnancy and send the relevant clinical investigations.
Common Signs and Symptoms
Signs and symptoms — The most common signs and symptoms of early pregnancy are:
Increased skin pigmentation (face, linea alba, areola)
Difficulty sleeping
Low back pain
Adnexal discomfort
In a study that prospectively collected data on the onset of pregnancy symptoms in 221 females attempting to conceive, 60 percent experienced some signs or symptoms of pregnancy as early as 5 to 6 weeks of gestation (ie, five to six weeks after the first day of their last menstrual period [LMP]), and 90 percent were symptomatic by 8 weeks.
Their symptoms tended to develop abruptly and occur daily. However, the symptoms were nonspecific: they also occurred in 9 percent of nonpregnant cycles.
Findings on physical examination
The pregnant uterus is more globular than in the nonpregnant state and enlarged, increasing in size by approximately 1 cm per week after 4 weeks of gestation. The correlation between uterine size and gestational age is often described in terms of fruit (eg, 6 to 8 week size = small pear; 8 to 10 week size = orange; 10 to 12 week size = grapefruit). The size of uterus can be guest by vaginal examination with bi-manual palpation method.
The uterus remains a pelvic organ until approximately 12 weeks of gestation when it becomes sufficiently large to palpate abdominally just above the symphysis pubis, unless the patient has obesity. At 16 weeks, the uterine fundus is palpable midway between the symphysis pubis and umbilicus.
The uterus and vaginal portion of the cervix soften beginning at approximately 6 weeks of gestation. Softening of the isthmus (lower portion of uterus adjacent to the cervix) allows the body of the uterus to flex against the cervix.
The mucous membranes of the vulva, vagina, and cervix become congested and may appear bluish (Chadwick sign) beginning at approximately 8 to 12 weeks of gestation.
The breasts become fuller and may become tender. The areola darkens, and the veins under the breast skin become more visible.
Fetal cardiac activity can usually be detected by a handheld Doppler device at 10 to 12 weeks of gestation and sometimes earlier if the patient is thin and the clinician is persistent (fetal heart size is <7 mm at 10 to 12 weeks.
UPT- Urine pregnancy test: Indication, Interpretatin, Normal Range
Table of Contents(toc)
Introduction
Pregnancy tests are essential tools for those trying to conceive or monitoring their reproductive health. One of the most common methods is the Urine Pregnancy Test (UPT), which is easy to use, widely available, and highly effective. In this article, we’ll explore the indications for using a UPT, how to interpret the results, and what constitutes a normal range.
signs of ppregnancy classification
Indications for a UPT
A Urine Pregnancy Test is typically indicated when:
Missed Period: If you have a regular menstrual cycle and miss your period, this is often the first sign to consider testing for pregnancy.
Early Pregnancy Symptoms: Symptoms such as nausea, breast tenderness, fatigue, and frequent urination can suggest pregnancy and warrant testing.
Contraceptive Failure: If you experience a failure of birth control methods (e.g., condom breakage), a UPT can confirm or rule out pregnancy.
Fertility Monitoring: Individuals or couples trying to conceive may use UPTs to check for pregnancy after unprotected intercourse.
Interpreting UPT Results
Interpreting a UPT is straightforward. Most tests come with clear instructions and can be done at home. Here’s how to understand the results:
Positive Result:
Two lines appear on the test strip, or a plus sign is visible. This indicates the presence of the hormone human chorionic gonadotropin (hCG), which is produced during pregnancy.
Negative Result:
One line appears, or the test shows a minus sign. This typically means that you are not pregnant, but testing too early can sometimes lead to false negatives.
Invalid Result: If no lines appear or the test does not function correctly, you should repeat the test with a new kit.
Normal Range
A UPT is designed to detect levels of hCG in urine, which begin to rise shortly after conception. A normal range for a positive result is generally any hCG level above 20-25 mIU/mL, although most tests can detect hCG at levels as low as 10 mIU/mL. For accurate results, it’s best to take the test after your missed period, as hCG levels will be more concentrated at that time.
Summary of urine pregnancy test
The Urine Pregnancy Test is a reliable and accessible method for confirming pregnancy. Knowing when to test, how to interpret the results, and understanding the normal range of hCG can empower you in your reproductive health journey.
Whether you are trying to conceive or monitoring your health, a UPT provides crucial information and peace of mind. Always consult a healthcare provider for further testing and confirmation following a positive result.
{
“@context”: “https://schema.org”,
“@type”: “FAQPage”,
“mainEntity”: [{
“@type”: “Question”,
“name”: “Indications for a UPT”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Missed Period: If you have a regular menstrual cycle and miss your period, this is often the first sign to consider testing for pregnancy.
Early Pregnancy Symptoms: Symptoms such as nausea, breast tenderness, fatigue, and frequent urination can suggest pregnancy and warrant testing.
Contraceptive Failure: If you experience a failure of birth control methods (e.g., condom breakage), a UPT can confirm or rule out pregnancy.
Fertility Monitoring: Individuals or couples trying to conceive may use UPTs to check for pregnancy after unprotected intercourse.”
}
},{
“@type”: “Question”,
“name”: “Normal range of serum Hcg”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “A normal range for a positive result is generally any hCG level above 20-25 mIU/mL, although most tests can detect hCG at levels as low as 10 mIU/mL.”
}
}]
}
Yuka is a perinneal shrub with wiidy tem from around southern and northern america.
Types of Yuka recipe
Different types of recipes are possible with Yuka plant. These are listed below.
Yuka fries
Yuka boiled
Yuka salad
Cakes
Pudding
Yuka fries recipe
Yuka fries is one of the famous recipe worldwide.
Steps of making yuka fries recipe
Yucca fries, also known as cassava fries, are a delicious and crispy alternative to traditional potato fries. Here are the steps to make yucca fries:
raw yuka before making yuka fries
Ingredients:
One large yucca root (cassava)
Vegetable oil, for frying
Salt, to taste
Optional: any preferred seasoning or spices (e.g., paprika, garlic powder, etc.)
Instructions:
Peel the yucca: Start by cutting off the ends of the yucca root with a sharp knife. Then, use a vegetable peeler or a knife to remove the thick, waxy skin from the yucca. Make sure to remove all the brown outer layer to reveal the white flesh inside.
Cut the yucca into fry shapes: Slice the yucca root in half lengthwise, and then cut each half into long, thin strips, just like you would cut regular potato fries. You can adjust the thickness according to your preference, but aim for relatively uniform sizes to ensure even cooking.
Boil the yucca: Fill a large pot with water and bring it to a boil. Add the yucca fries to the boiling water and cook for about 5-7 minutes until they are partially cooked but still firm. This step helps to soften the yucca and speeds up the frying process.
Drain and cool: Drain the partially cooked yucca fries in a colander and let them cool down for a few minutes. This will help remove excess moisture from the surface, making them crispier when fried.
Preheat the oil: In a deep fryer or a large, heavy-bottomed pot, add enough vegetable oil to submerge the yucca fries completely. Preheat the oil to around 350°F (175°C). If you don’t have a thermometer, you can test the oil readiness by adding a small piece of yucca; it should sizzle immediately without burning.
Yuca fries french fries
Fry the yucca: Carefully add the yucca fries to the hot oil in batches to avoid overcrowding the fryer. Fry them for about 3-5 minutes or until they turn golden brown and crispy. Stir them occasionally during frying to ensure even cooking.
Drain and season: Using a slotted spoon, remove the fried yucca fries from the oil and place them on a plate lined with paper towels to drain any excess oil. Immediately sprinkle them with salt and any other desired seasoning while they are still hot.
Serve and enjoy: Yucca fries are best enjoyed immediately while they are still hot and crispy. Serve them as a delicious side dish or a snack, and optionally pair them with your favorite dipping sauce or salsa.
Enjoy your homemade yucca fries!
Nutritional values off yuca fries
(per serving of around 100 gram)
Total Calories: 300 calories
Fat: 25%
saturated fat 8%
Cholesterl: 0%
Sodium: 12 gm
Total carbohydrate: 12%
Dietary fiber: 6%
Protein: 1.2gram
Potassium: 240 mg
Vitamins and minerals: Vitamin A, C and E, Iron, calcium and selenium available.
If you’re looking for a healthy and tasty alternative to potatoes, yuca or cassava might be just what you need. This starchy root vegetable, also known as manioc, is a staple food in many parts of the world, from South America and Africa to Asia and the Caribbean. But is yuca or cassava healthy? And what are some of the most popular ways to cook and serve it? Let’s find out.
Yuca or cassava is a great source of carbohydrates, fiber, and various vitamins and minerals. Here are some of the health benefits of this versatile root vegetable:
Yuca or cassava is rich in resistant starch, which can improve digestive health, lower blood sugar levels, and promote satiety and weight loss.
Yuca or cassava is a good source of vitamin C, which can boost immunity, collagen production, and iron absorption.
Yuca or cassava is a decent source of potassium, which can regulate blood pressure, fluid balance, and muscle function.
Yuca or cassava is low in fat and cholesterol, which can benefit heart health and overall health.
However, it’s worth noting that yuca or cassava also contains cyanide, a toxic substance that can cause poisoning if consumed in large amounts. To avoid this risk, make sure to peel and cook yuca or cassava properly before eating it.
Classification: setting in which the person has contracted their infection
Community-acquired pneumonia (CAP) definition :
It occurs outside hospital setting or less than 48 hours after admission
Hospital-acquired pneumonia (HAP):
Hospital-acquired or nosocomial pneumonia refers to a new episode of pneumonia occurring at least 2 days after admission to hospital.
Contd…
Health care-associated pneumonia (HCAP) :
refers to the development of pneumonia in a person who has spent at least 2 days in hospital within the last 90 days, attended a haemodialysis unit, received intravenous antibiotics, or been resident in a nursing home or other long-term care facility.
Immunocompromised host :
Neutropenic, HIV +, Cancer,Mycobacterium tuberculosis, Pneumocystis jiroveci ,Immunosuppressives
Classification by site of pneumonia
Lobar pnemonia :
Infection can be localized with the whole of one or more lobes affected. >90% of the cases is due to Strep.pneumoniae
Influenza vaccination is recommended to those at high risk of mortality from influenza or pneumonia
All patients over the age of 65 who have not previously been vaccinated and are admitted with CAP should have the pneumococcal vaccine before discharge
Pneumonia MCQs
Dr Chaitanya
1
Most common symptom of the respiratory disease is?
a) Wheeze
b) Cough
c) Fever
d) Hemoptysis
Ans:
B cough
2
Common sound heard on auscultation in pneumonia is
•Rales
•Ronchi
•Wheeze
•Crackles
crackles
3
An old man comes to u with complaint of fever for 4 days and cough associated with chills. On examination the patient is in respiratory distress and AND HAS HIGH GRADE FEVER OF 104 DEGREE FAHRENHEIT. The most possible diagnosis is
•COPD
•PTB
•Bronchial asthma
•Pneumonia
Pneumonia
4
A pus sample is called purulent if
Pneumonia depiction
•Pus cells > 25 and epithelial cells < 10
•Pus cells > 15 and epithelial cells < 5
•Pus cells > 30 and epithelial cells < 10
•Pus cells > 20 and epithelial cells < 5
A. Pus cells > 25 and epithelial cells < 10
5
A patient who is known case of COPD under medication has complained of increased shortness of breath. He said that he could walk on plane level with his friends easily but now he needs to take break every 100 m or so due to shortness of breath. What is the mMRC grade of SOB for this patient?
1
2
3
4
0
3
6 Difficulty in breathing is called
Dyspnoea
Orthopnoea
Tachypnoea
Apnoea
Dyspnoea
7
Which organism causes the so called walking pneumonia (Hint: atypical pneumonia)
Streptococcus
Klebsiella
H1n1
SARS-CoV2
Mycoplasma
Mycoplasma
8
HAP is called if symptoms/diagnosis
Within 2 days of admission
After 48 hours of admission
2 days of admission to 2 days of discharge
If patient admitted to ICU
2 days of admission to 2 days of discharge
9
Common causative agent for congenital or neonatal oneumonia is
H. influenziae
Chlamydia pneumoniae
Streptococcus pneumoniae
Broup B streptococcus
Gr. B strep
10
In CURB 65 scoring B stands for
Blood urea nitrogen
Blood count
Blood pressure
Breathing
Blood pressure ( sys<90 or dias <60)
11
Lung abscess following pneumonia is caused by
Staphylococcus
Streptococcus
Pneumocystis
Coronavirus
Staphylococcus
12
Antibiotic of choice for CAP in OPD setting is
Amoxycillin
Ciprofloxacin
Metronidazole
Doxycycline
Amoxycillin
13
Pneumothorax is
Hyperexpansion of lungs
Air in thoracic cavity
No breathing by lungs
Lung mixed with ait
Air in thoracic cavity
14
Your patient has BP of 130/90 mm of Hg. What is his MAP
Mycoplasma pneumonia : The dangerous walking talking pneumonia
Table of Contents (toc)
Introduction
Mycoplasma pneumonia is a common cause of respiratory tract infections in
adolescents. It can present with fever, cough, and infiltrates on chest X-ray.
In some cases, mycoplasma infection can also cause skin manifestations such as
vesicles or blisters.
Presenting symtoms of mycoplasma pneumonia
The patient is presenting with symptoms suggestive of Mycoplasma pneumonia,
including fever, cough, and infiltrates on chest X-ray. The presence of
vesicles or blisters on the skin further supports the possibility of
Mycoplasma-induced skin manifestations.
57.Following drugs are effective against Mycoplasma pneumoniae except:
Antimicrobial activity of Amoxycillin is via inhibition of cell wall synthesis which has no role in Mycoplasma.
Penicillin ineffective since mycoplasma have no cell wall.
Treatment (Mycoplasma)
Macrolides
Doxycycline or
Fluoroquinolone
3
MOA
Macrolides
Clarithromycin
Azithromycion
inhibit protein synthesis by blocking translocation: blinds to 23srRNA of 50s ribosomal subunit
Bacteriostatic
Tetracyclines
Tetracycline
Doxycycline
Bind to 30S & prevent attachment of aminoacyl-t RNA Bacteriostatic
Rifamycin
Rifampin
Inhibit DNA dependent RNA polymerase
Rifabutin
Fluroquinolones
Ciprofloxacin
Norfloxacin
Levofloxacin
Inhibit prokaryotic
enzymes topo isomerase II (DNA gyrase) & topoisomerase IV.
FAQs:
1. Can Mycoplasma pneumonia cause skin manifestations?
Yes, in some cases, Mycoplasma pneumonia can cause skin manifestations such as
vesicles or blisters.
2. How is Mycoplasma pneumonia diagnosed?
Mycoplasma pneumonia can be diagnosed through serological testing for
Mycoplasma antibodies or PCR testing for Mycoplasma DNA in respiratory
samples.
3. What is the treatment for Mycoplasma pneumonia?
The treatment for Mycoplasma pneumonia involves the use of antibiotics such as
macrolides or tetracyclines.
4. Is Mycoplasma pneumonia contagious?
Yes, Mycoplasma pneumonia is contagious and can spread through respiratory
droplets.
5. Can Mycoplasma pneumonia cause complications?
Yes, Mycoplasma pneumonia can lead to complications such as pneumonia,
bronchitis, or ear infections.
{
“@context”: “https://schema.org”,
“@type”: “FAQPage”,
“mainEntity”: [{
“@type”: “Question”,
“name”: “1. Can Mycoplasma pneumonia cause skin manifestations?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Yes, in some cases, Mycoplasma pneumonia can cause skin manifestations such as vesicles or blisters.”
}
},{
“@type”: “Question”,
“name”: “2. How is Mycoplasma pneumonia diagnosed?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Mycoplasma pneumonia can be diagnosed through serological testing for Mycoplasma antibodies or PCR testing for Mycoplasma DNA in respiratory samples.”
}
},{
“@type”: “Question”,
“name”: “3. What is the treatment for Mycoplasma pneumonia?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “The treatment for Mycoplasma pneumonia involves the use of antibiotics such as macrolides or tetracyclines.”
}
},{
“@type”: “Question”,
“name”: “4. Is Mycoplasma pneumonia contagious?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Yes, Mycoplasma pneumonia is contagious and can spread through respiratory droplets.”
}
},{
“@type”: “Question”,
“name”: “5. Can Mycoplasma pneumonia cause complications?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Yes, Mycoplasma pneumonia can lead to complications such as pneumonia, bronchitis, or ear infections.”
}
}]
}
Stay Connected with Dr. Chaitanya Joshi, MD
YouTube Channel
Watch health videos, tips, and updates from Dr. Chaitanya MD.