Yuka is a perinneal shrub with wiidy tem from around southern and northern america.
Types of Yuka recipe
Different types of recipes are possible with Yuka plant. These are listed below.
Yuka fries
Yuka boiled
Yuka salad
Cakes
Pudding
Yuka fries recipe
Yuka fries is one of the famous recipe worldwide.
Steps of making yuka fries recipe
Yucca fries, also known as cassava fries, are a delicious and crispy alternative to traditional potato fries. Here are the steps to make yucca fries:
raw yuka before making yuka fries
Ingredients:
One large yucca root (cassava)
Vegetable oil, for frying
Salt, to taste
Optional: any preferred seasoning or spices (e.g., paprika, garlic powder, etc.)
Instructions:
Peel the yucca: Start by cutting off the ends of the yucca root with a sharp knife. Then, use a vegetable peeler or a knife to remove the thick, waxy skin from the yucca. Make sure to remove all the brown outer layer to reveal the white flesh inside.
Cut the yucca into fry shapes: Slice the yucca root in half lengthwise, and then cut each half into long, thin strips, just like you would cut regular potato fries. You can adjust the thickness according to your preference, but aim for relatively uniform sizes to ensure even cooking.
Boil the yucca: Fill a large pot with water and bring it to a boil. Add the yucca fries to the boiling water and cook for about 5-7 minutes until they are partially cooked but still firm. This step helps to soften the yucca and speeds up the frying process.
Drain and cool: Drain the partially cooked yucca fries in a colander and let them cool down for a few minutes. This will help remove excess moisture from the surface, making them crispier when fried.
Preheat the oil: In a deep fryer or a large, heavy-bottomed pot, add enough vegetable oil to submerge the yucca fries completely. Preheat the oil to around 350°F (175°C). If you don’t have a thermometer, you can test the oil readiness by adding a small piece of yucca; it should sizzle immediately without burning.
Yuca fries french fries
Fry the yucca: Carefully add the yucca fries to the hot oil in batches to avoid overcrowding the fryer. Fry them for about 3-5 minutes or until they turn golden brown and crispy. Stir them occasionally during frying to ensure even cooking.
Drain and season: Using a slotted spoon, remove the fried yucca fries from the oil and place them on a plate lined with paper towels to drain any excess oil. Immediately sprinkle them with salt and any other desired seasoning while they are still hot.
Serve and enjoy: Yucca fries are best enjoyed immediately while they are still hot and crispy. Serve them as a delicious side dish or a snack, and optionally pair them with your favorite dipping sauce or salsa.
Enjoy your homemade yucca fries!
Nutritional values off yuca fries
(per serving of around 100 gram)
Total Calories: 300 calories
Fat: 25%
saturated fat 8%
Cholesterl: 0%
Sodium: 12 gm
Total carbohydrate: 12%
Dietary fiber: 6%
Protein: 1.2gram
Potassium: 240 mg
Vitamins and minerals: Vitamin A, C and E, Iron, calcium and selenium available.
If you’re looking for a healthy and tasty alternative to potatoes, yuca or cassava might be just what you need. This starchy root vegetable, also known as manioc, is a staple food in many parts of the world, from South America and Africa to Asia and the Caribbean. But is yuca or cassava healthy? And what are some of the most popular ways to cook and serve it? Let’s find out.
Yuca or cassava is a great source of carbohydrates, fiber, and various vitamins and minerals. Here are some of the health benefits of this versatile root vegetable:
Yuca or cassava is rich in resistant starch, which can improve digestive health, lower blood sugar levels, and promote satiety and weight loss.
Yuca or cassava is a good source of vitamin C, which can boost immunity, collagen production, and iron absorption.
Yuca or cassava is a decent source of potassium, which can regulate blood pressure, fluid balance, and muscle function.
Yuca or cassava is low in fat and cholesterol, which can benefit heart health and overall health.
However, it’s worth noting that yuca or cassava also contains cyanide, a toxic substance that can cause poisoning if consumed in large amounts. To avoid this risk, make sure to peel and cook yuca or cassava properly before eating it.
Classification: setting in which the person has contracted their infection
Community-acquired pneumonia (CAP) definition :
It occurs outside hospital setting or less than 48 hours after admission
Hospital-acquired pneumonia (HAP):
Hospital-acquired or nosocomial pneumonia refers to a new episode of pneumonia occurring at least 2 days after admission to hospital.
Contd…
Health care-associated pneumonia (HCAP) :
refers to the development of pneumonia in a person who has spent at least 2 days in hospital within the last 90 days, attended a haemodialysis unit, received intravenous antibiotics, or been resident in a nursing home or other long-term care facility.
Immunocompromised host :
Neutropenic, HIV +, Cancer,Mycobacterium tuberculosis, Pneumocystis jiroveci ,Immunosuppressives
Classification by site of pneumonia
Lobar pnemonia :
Infection can be localized with the whole of one or more lobes affected. >90% of the cases is due to Strep.pneumoniae
Influenza vaccination is recommended to those at high risk of mortality from influenza or pneumonia
All patients over the age of 65 who have not previously been vaccinated and are admitted with CAP should have the pneumococcal vaccine before discharge
Pneumonia MCQs
Dr Chaitanya
1
Most common symptom of the respiratory disease is?
a) Wheeze
b) Cough
c) Fever
d) Hemoptysis
Ans:
B cough
2
Common sound heard on auscultation in pneumonia is
•Rales
•Ronchi
•Wheeze
•Crackles
crackles
3
An old man comes to u with complaint of fever for 4 days and cough associated with chills. On examination the patient is in respiratory distress and AND HAS HIGH GRADE FEVER OF 104 DEGREE FAHRENHEIT. The most possible diagnosis is
•COPD
•PTB
•Bronchial asthma
•Pneumonia
Pneumonia
4
A pus sample is called purulent if
Pneumonia depiction
•Pus cells > 25 and epithelial cells < 10
•Pus cells > 15 and epithelial cells < 5
•Pus cells > 30 and epithelial cells < 10
•Pus cells > 20 and epithelial cells < 5
A. Pus cells > 25 and epithelial cells < 10
5
A patient who is known case of COPD under medication has complained of increased shortness of breath. He said that he could walk on plane level with his friends easily but now he needs to take break every 100 m or so due to shortness of breath. What is the mMRC grade of SOB for this patient?
1
2
3
4
0
3
6 Difficulty in breathing is called
Dyspnoea
Orthopnoea
Tachypnoea
Apnoea
Dyspnoea
7
Which organism causes the so called walking pneumonia (Hint: atypical pneumonia)
Streptococcus
Klebsiella
H1n1
SARS-CoV2
Mycoplasma
Mycoplasma
8
HAP is called if symptoms/diagnosis
Within 2 days of admission
After 48 hours of admission
2 days of admission to 2 days of discharge
If patient admitted to ICU
2 days of admission to 2 days of discharge
9
Common causative agent for congenital or neonatal oneumonia is
H. influenziae
Chlamydia pneumoniae
Streptococcus pneumoniae
Broup B streptococcus
Gr. B strep
10
In CURB 65 scoring B stands for
Blood urea nitrogen
Blood count
Blood pressure
Breathing
Blood pressure ( sys<90 or dias <60)
11
Lung abscess following pneumonia is caused by
Staphylococcus
Streptococcus
Pneumocystis
Coronavirus
Staphylococcus
12
Antibiotic of choice for CAP in OPD setting is
Amoxycillin
Ciprofloxacin
Metronidazole
Doxycycline
Amoxycillin
13
Pneumothorax is
Hyperexpansion of lungs
Air in thoracic cavity
No breathing by lungs
Lung mixed with ait
Air in thoracic cavity
14
Your patient has BP of 130/90 mm of Hg. What is his MAP
Mycoplasma pneumonia : The dangerous walking talking pneumonia
Table of Contents (toc)
Introduction
Mycoplasma pneumonia is a common cause of respiratory tract infections in
adolescents. It can present with fever, cough, and infiltrates on chest X-ray.
In some cases, mycoplasma infection can also cause skin manifestations such as
vesicles or blisters.
Presenting symtoms of mycoplasma pneumonia
The patient is presenting with symptoms suggestive of Mycoplasma pneumonia,
including fever, cough, and infiltrates on chest X-ray. The presence of
vesicles or blisters on the skin further supports the possibility of
Mycoplasma-induced skin manifestations.
57.Following drugs are effective against Mycoplasma pneumoniae except:
Antimicrobial activity of Amoxycillin is via inhibition of cell wall synthesis which has no role in Mycoplasma.
Penicillin ineffective since mycoplasma have no cell wall.
Treatment (Mycoplasma)
Macrolides
Doxycycline or
Fluoroquinolone
3
MOA
Macrolides
Clarithromycin
Azithromycion
inhibit protein synthesis by blocking translocation: blinds to 23srRNA of 50s ribosomal subunit
Bacteriostatic
Tetracyclines
Tetracycline
Doxycycline
Bind to 30S & prevent attachment of aminoacyl-t RNA Bacteriostatic
Rifamycin
Rifampin
Inhibit DNA dependent RNA polymerase
Rifabutin
Fluroquinolones
Ciprofloxacin
Norfloxacin
Levofloxacin
Inhibit prokaryotic
enzymes topo isomerase II (DNA gyrase) & topoisomerase IV.
FAQs:
1. Can Mycoplasma pneumonia cause skin manifestations?
Yes, in some cases, Mycoplasma pneumonia can cause skin manifestations such as
vesicles or blisters.
2. How is Mycoplasma pneumonia diagnosed?
Mycoplasma pneumonia can be diagnosed through serological testing for
Mycoplasma antibodies or PCR testing for Mycoplasma DNA in respiratory
samples.
3. What is the treatment for Mycoplasma pneumonia?
The treatment for Mycoplasma pneumonia involves the use of antibiotics such as
macrolides or tetracyclines.
4. Is Mycoplasma pneumonia contagious?
Yes, Mycoplasma pneumonia is contagious and can spread through respiratory
droplets.
5. Can Mycoplasma pneumonia cause complications?
Yes, Mycoplasma pneumonia can lead to complications such as pneumonia,
bronchitis, or ear infections.
{
“@context”: “https://schema.org”,
“@type”: “FAQPage”,
“mainEntity”: [{
“@type”: “Question”,
“name”: “1. Can Mycoplasma pneumonia cause skin manifestations?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Yes, in some cases, Mycoplasma pneumonia can cause skin manifestations such as vesicles or blisters.”
}
},{
“@type”: “Question”,
“name”: “2. How is Mycoplasma pneumonia diagnosed?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Mycoplasma pneumonia can be diagnosed through serological testing for Mycoplasma antibodies or PCR testing for Mycoplasma DNA in respiratory samples.”
}
},{
“@type”: “Question”,
“name”: “3. What is the treatment for Mycoplasma pneumonia?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “The treatment for Mycoplasma pneumonia involves the use of antibiotics such as macrolides or tetracyclines.”
}
},{
“@type”: “Question”,
“name”: “4. Is Mycoplasma pneumonia contagious?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Yes, Mycoplasma pneumonia is contagious and can spread through respiratory droplets.”
}
},{
“@type”: “Question”,
“name”: “5. Can Mycoplasma pneumonia cause complications?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Yes, Mycoplasma pneumonia can lead to complications such as pneumonia, bronchitis, or ear infections.”
}
}]
}
Urinary tract infections and calculus UTI and renal stones (nepphrolithiasis), bladder stones
Table of contents (toc)
Introduction to UTI
A urinary tract infection (UTI) is an infection in any part of the urinary system, which includes the kidneys, ureters, bladder, and urethra. Most infections involve the lower urinary tract, specifically the bladder and urethra. UTIs are typically caused by bacteria, most commonly Escherichia coli (E. coli), that enter the urinary tract through the urethra and begin to multiply in the bladder.
Symptoms of uti
Symptoms of a UTI can include a strong, persistent urge to urinate, a burning sensation when urinating, passing frequent, small amounts of urine, urine that appears cloudy, or urine that has a strong odor. If the infection spreads to the kidneys, it can cause more severe symptoms, including fever, back pain, and nausea.
Treatment of UTI
UTIs are more common in women than in men, and they can usually be treated effectively with antibiotics.
Introduction to Nephrolithiasis
Nephrolithiasis, commonly known as kidney stones, refers to the formation of hard mineral and salt deposits in the kidneys. These stones can vary in size and may develop when urine becomes concentrated, allowing minerals to crystallize and stick together.
Symptoms of kidney stones
Kidney stones can cause severe pain when they pass through the urinary tract. Symptoms may include intense pain in the back or side, pain during urination, blood in the urine, and sometimes nausea and vomiting. The pain often starts suddenly and may come in waves as the stone moves.
Type of kidney stones
The main types of kidney stones include calcium stones (the most common type), struvite stones (which can form after a urinary tract infection), uric acid stones, and cystine stones (which are rare and usually occur in people with a genetic disorder).
Treatment of kidney stones
Treatment for nephrolithiasis depends on the size and type of stone. Smaller stones may pass on their own with increased fluid intake and pain management, while larger stones may require medical intervention, such as extracorporeal shock wave lithotripsy (ESWL) to break the stone into smaller pieces, or surgical removal. Preventative measures often include dietary adjustments and medications to reduce the risk of recurrence.
Introduction of urethral dilation in female: 30 causes of painful intercourse
Table of Contents(toc)
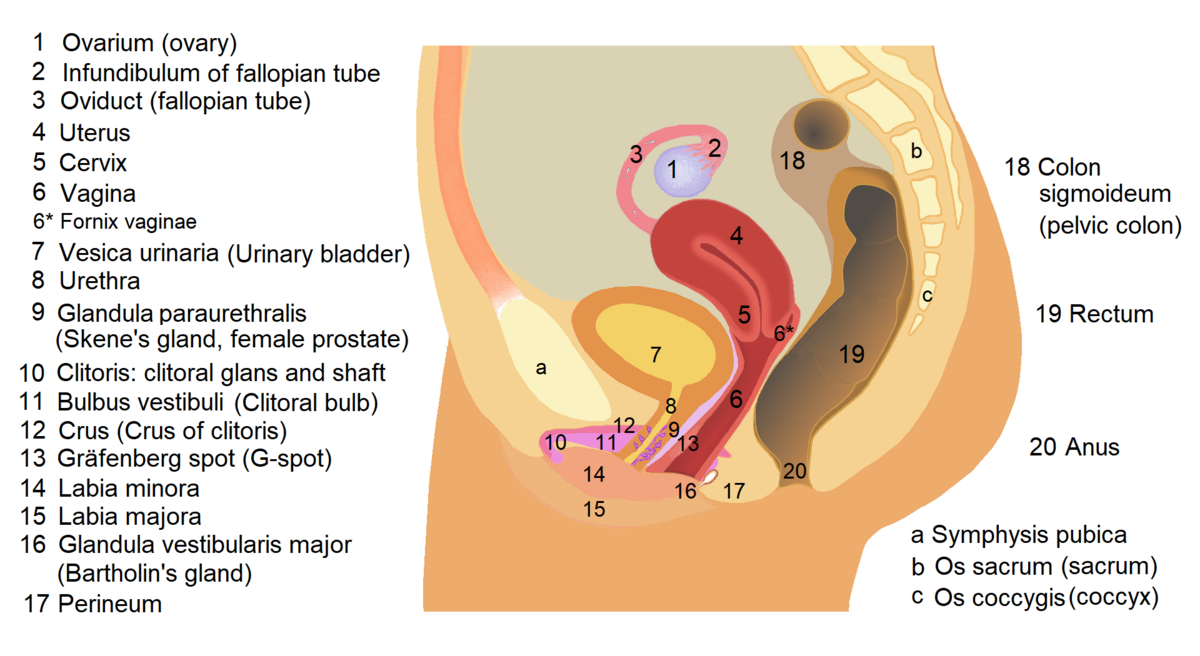
female genitourinary system
Urethra dilation is a delicate medical procedure done underanesthesis by a urologist or urosurgeon. The procedure is done after careful evaluation and by well trained professionals. Before going deeper into female urethra dilation lets review anatomy of female urethra in brief.
Urethral structure if pathological narrowing of urethra due to different reasons leading to difficulty passing urine and various other symptoms and consequences.
Anatomy of female urethra
Female urethra is tubular musculocutaneous organelle situation in genital region of female that connects bladder to the outer world. The urethra carries urine from bladder to the outside. The flow of urine from bladder is controlled by two valves viz. Internal and external urethral valves. The internal urethral valve is controlled by autonomic nervous system while external is under voluntary control. The overall length of fenale urethra is 4 centimetres or 1.5 inches.
(Source: Textbook of anatomy 7e, Moore et al. )
Female urinary system anatomy
Indications of urethral dilation : an introduction
Sexual intercourse after female urrthra dilatation may become difficult rarely. Difficult or painful sexual intercourse is called dysparaunia and it may have several other causes including vaginal infection, dry vagina and many more listed as below.
Painful sexual intercourse or dyspareunia can be because of external genital problems to internal vaginal, uterine or pelvic disorders. Urethra also being near vagina can be the reason for dyspareunia where as other nearby organs and structures can also be part of it. It is also called genitopelvic pain. The causes of painful intercourse can be listed as below:
The flow of urine from bladder is controlled by two valves viz. Internal and external urethral valves. The internal urethral valve is controlled by autonomic nervous system while external is under voluntary control.
Extreme female urethra dikagyrefers to dilating urethra above the normal anatomical diameter as expected of that age.
This will be done in case of following indications
Lecture on Aseptic Meningitis (Viral Meningitis) lecture 2025
Table of contents (toc)
Aseptic Meningitis (Viral Meningitis)
Definition of aseptic meningitis:
Aseptic meningitis is a clinical term for an illness comprising meningeal
irritation, fever, and alterations in consciousness of relatively acute
onset.
Shock and Burn Powerpoint PPT : Loksewa, NMCLE, NNC, NHPC and MDMS MEC
Table of Contents(toc)
Introduction
Fire accidents are common type of injuries that happen in world daily basis.
Shock is a clinical condition that results due to inadequate tissue perfusion.
A critical condition brought on by the sudden drop in blood flow through the body.
May result from trauma, heatstroke, blood loss, an allergic reaction, severe infection, poisoning, severe burns or other causes.
Occurs when the metabolic needs of cells are not met because of inadequate blood flow.
These two topics are very common in emergency managent and should be well taught to medical students, graduates and paramedics.
Signs and symptoms
Cool, clammy skin
Pale or ashen skin
Bluish tinge to lips or fingernails (or gray in the case of dark complexions)
Rapid pulse
Rapid breathing
Nausea or vomiting
Enlarged pupils
Weakness or fatigue
Dizziness or fainting
Changes in mental status or behavior, such as anxiousness or agitation
Burn with Fire
Types of Shock
Hypovolemic Shock
Cardiogenic Shock
Neurogenic Shock
Anaphylatic Shock
Septic Shock
Introduction to BURN
Burns are tissue damage that results from heat, overexposure to the sun or other radiation, or chemical or electrical contact.
Wound with destruction of tissue due to coagulation necrosis.
Causes of burn
Thermal burn/heat burn: dry heat
Scald: moist heat
Electric burn: electricity
Cold burn: frost bite
Chemical burn: strong acid and alkali
Radiation burn: X-rays, Gamma rays
Degree of Burn Classification and grading
First degree – superficial thickness
Second degree – Partial or intermediate thickenss
Third degree – Full thickness
Fourth degree
Management of burn
Remove burning source immediately.
Wrap the patient in a cloth and roll him in the floor.
Immerse 10-15 minutesin water or cool down the burnt part in running water for 15 minutes
Give liquids orally. Provide analgesics and antibiotics.
Do not rupture blister.
TT injection
First-degree burns:
Run cool water over the burn. Don’t apply ice. For sunburns, apply aloe vera gel. For thermal burns, apply antibiotic cream and cover lightly with gauze. You can also take over-the-counter pain medication.
Second-degree burns:
Treatment for second- and first-degree burns is similar.
Stronger antibiotic – such as silver sulfadiazine, to kill bacteria
Elevating the burned area can reduce pain and swelling.
May need dressing to be applied
Third-degree burns:
Third-degree burns can belife-threatening and often require skin grafts. Skin grafts replace damaged tissue with healthy skin from another of the uninjured part of the person’s body.
Wallace Rule of Nine
The Wallace Rule of Nines is a method used to estimate the total body surface area (TBSA) affected by burns. It divides the body into sections, each representing approximately 9% (or multiples thereof) of the total body surface area. The distribution is slightly different for adults and children due to differences in body proportions.
Wallace Rule of Nines for Adults:
Head and Neck: 9%
Each Arm: 9% (4.5% front, 4.5% back)
Each Leg: 18% (9% front, 9% back)
Anterior Torso (Chest and Abdomen): 18%
Posterior Torso (Back and Buttocks): 18%
Perineum/Genitalia: 1%
Wallace Rule of Nines for Children:
Head and Neck: 18% (larger proportion due to the relatively larger head size in children)
Each Arm: 9% (4.5% front, 4.5% back)
Each Leg: 14% (7% front, 7% back; less than in adults because legs are relatively shorter)
Anterior Torso (Chest and Abdomen): 18%
Posterior Torso (Back and Buttocks): 18%
Perineum/Genitalia: 1%
These percentages are used to help us quickly estimate the extent of burns and its severity, which is critical for determining the severity of the injury and guiding treatment decisions, such as fluid resuscitation and transfer to a specialized burn center.
Parkland Formula:
The Parkland formula, also known as the Baxter formula, is used to calculate the amount of fluid required for resuscitation in burn patients within the first 24 hours after injury. The formula is based on the patient’s weight and the total body surface area (TBSA) burned.
Total fluid requirement:4 mL×body weight (kg)×% TBSA burned4 , text{mL} times text{body weight (kg)} times text{% TBSA burned}
4mL×body weight (kg)×% TBSA burned
Administration:
First 8 hours: Administer half of the total fluid requirement.
Next 16 hours: Administer the remaining half.
Example for an Adult:
If an adult weighs 70 kg and has 30% TBSA burns:
Total fluid requirement:4×70×30=8,400 mL4 times 70 times 30 = 8,400 , text{mL}4×70×30=8,400mL
First 8 hours:8,400/2=4,200 mL8,400 / 2 = 4,200 , text{mL}8,400/2=4,200mL
Next 16 hours:4,200 mL4,200 , text{mL}4,200mL
The Parkland formula provides an initial guideline for fluid resuscitation, but ongoing assessment and adjustments based on the patient’s clinical response (urine output, vital signs, etc.) are critical for effective management.
OTHER CONCEPTs on bubrn management
Patient may require IV antibiotics for infection prevention/control
If oral intake not possible IV fluids till oral can be started
{
“@context”: “https://schema.org”,
“@type”: “FAQPage”,
“mainEntity”: [{
“@type”: “Question”,
“name”: “What are Signs and symptoms of Burn?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Cool, clammy skin
Pale or ashen skin
Bluish tinge to lips or fingernails (or gray in the case of dark complexions)
Rapid pulse
Rapid breathing
Nausea or vomiting
Enlarged pupils
Weakness or fatigue
Dizziness or fainting”
}
},{
“@type”: “Question”,
“name”: “What are Types of Shock?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Hypovolemic Shock
Cardiogenic Shock
Neurogenic Shock
Anaphylatic Shock
Septic Shock”
}
},{
“@type”: “Question”,
“name”: “What are causes of Burn?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Thermal burn/heat burn: dry heat
Scald: moist heat
Electric burn: electricity
Cold burn: frost bite
Chemical burn: strong acid and alkali
Radiation burn: X-rays, Gamma rays”
}
},{
“@type”: “Question”,
“name”: “What is clasification of burn?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “First degree – superficial thickness
Second degree – Partial or intermediate thickenss
Third degree – Full thickness
Fourth degree”
}
},{
“@type”: “Question”,
“name”: “What is Management of burn?”,
“acceptedAnswer”: {
“@type”: “Answer”,
“text”: “Remove burning source immediately.
Wrap the patient in a cloth and roll him in the floor.
Immerse 10-15 minutes in water or cool down the burnt part in running water for 15 minutes
Give liquids orally. Provide analgesics and antibiotics.
Do not rupture blister.
TT injection
First-degree burns:
Run cool water over the burn. Don’t apply ice. For sunburns, apply aloe vera gel. For thermal burns, apply antibiotic cream and cover lightly with gauze. You can also take over-the-counter pain medication.
Second-degree burns:
Treatment for second- and first-degree burns is similar.
Stronger antibiotic – such as silver sulfadiazine, to kill bacteria
Elevating the burned area can reduce pain and swelling.
May need dressing to be applied
Third-degree burns:
Third-degree burns can be life-threatening and often require skin grafts. Skin grafts replace damaged tissue with healthy skin from another of the uninjured part of the person’s body.”
}
}]
}
Stay Connected with Dr. Chaitanya Joshi, MD
YouTube Channel
Watch health videos, tips, and updates from Dr. Chaitanya MD.