Table of Contents
Introduction
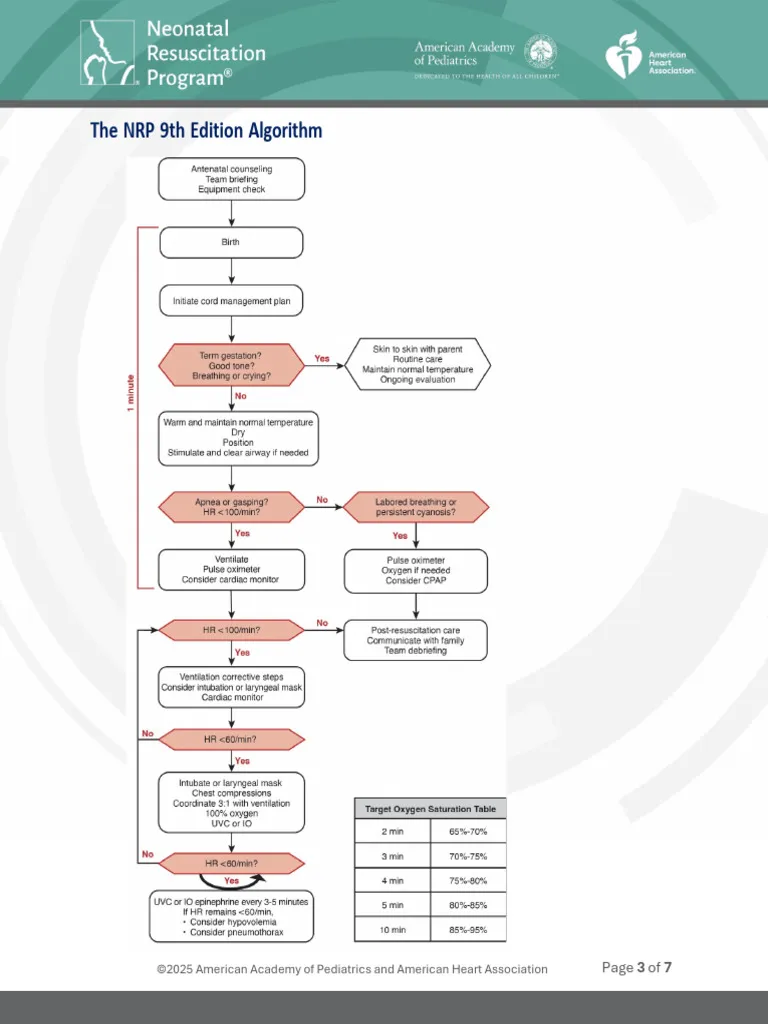
Neonatal resuscitation is one of the most time-sensitive and high-stakes procedures in pediatrics. Despite structured guidelines like the American Academy of Pediatrics and the Neonatal Resuscitation Program, errors still occur—even among experienced clinicians.
These mistakes can lead to preventable morbidity and mortality. Understanding them is essential not only for pediatricians but also for residents, nurses, and delivery room staff.
In this article, we’ll break down 5 common mistakes pediatricians make during neonatal resuscitation and how to correct them using evidence-based practice.
1. Delayed Initiation of Positive Pressure Ventilation (PPV)
❌ The Mistake
Failure to initiate Positive Pressure Ventilation (PPV) within the “Golden Minute” when the neonate is apneic, gasping, or has a heart rate <100 bpm.
⚠️ Why It Matters
- Ventilation—not chest compressions—is the most critical intervention
- Delays increase risk of:
- Hypoxic-ischemic injury
- Bradycardia progression
- Poor neurological outcomes
✅ Best Practice
- Assess breathing and heart rate immediately after birth
- Start PPV within 60 seconds (“Golden Minute”)
- Use pulse oximetry early
2. Inadequate Mask Seal and Poor Ventilation Technique
❌ The Mistake
- Improper mask size or seal
- Incorrect head positioning
- Ineffective ventilation despite apparent effort
⚠️ Why It Matters
- Most failed resuscitations are due to ineffective ventilation
- Leads to persistent hypoxia and bradycardia
✅ Best Practice (MR SOPA Approach)
Follow the MR SOPA corrective steps:
- Mask adjustment
- Reposition airway
- Suction mouth and nose
- Open mouth
- Pressure increase
- Airway alternative (ET tube or LMA)
3. Premature Initiation of Chest Compressions
❌ The Mistake
Starting chest compressions before ensuring adequate ventilation
⚠️ Why It Matters
- Neonatal cardiac arrest is usually respiratory in origin
- Without proper ventilation:
- Compressions are ineffective
- Oxygen delivery remains inadequate
✅ Best Practice
- Ensure effective ventilation for at least 30 seconds
- Start compressions only if:
- HR <60 bpm despite effective PPV
4. Incorrect Oxygen Use (Too Much or Too Little)
❌ The Mistake
- Starting all neonates on 100% oxygen
- Failure to titrate oxygen using pulse oximetry
⚠️ Why It Matters
- Hyperoxia → oxidative stress, especially in preterms
- Hypoxia → organ damage
✅ Best Practice
- Term babies: start with 21% oxygen (room air)
- Preterm babies: start with 21–30% oxygen
- Adjust based on preductal SpO₂ targets
5. Poor Team Communication and Role Assignment
❌ The Mistake
- Lack of clear leadership
- Unassigned roles
- Ineffective communication during resuscitation
⚠️ Why It Matters
- Leads to:
- Delayed interventions
- Duplicate or missed actions
- Increased stress and errors
✅ Best Practice
- Assign roles before delivery:
- Airway manager
- Compressor
- Medication nurse
- Team leader
- Use closed-loop communication
- Conduct pre-resuscitation briefing
Pro Tips for Better Neonatal Resuscitation
- Always prepare equipment before delivery
- Anticipate high-risk deliveries
- Use checklists
- Practice simulation training regularly
- Follow updates from American Heart Association
Conclusion
Even skilled pediatricians can make errors during neonatal resuscitation—but most are preventable. The key lies in:
- Mastering ventilation techniques
- Following structured protocols
- Practicing teamwork and communication
By avoiding these common mistakes, clinicians can significantly improve neonatal outcomes and reduce mortality.
FAQs
What is the most common mistake in neonatal resuscitation?
The most common mistake is ineffective ventilation due to poor mask seal or technique.
When should chest compressions be started in neonates?
Only when the heart rate is below 60 bpm after 30 seconds of effective ventilation.
Why is oxygen titration important in newborn resuscitation?
Both hypoxia and hyperoxia are harmful, especially in preterm infants.