Table of Contents
What is Acute Hepatic Failure?
Acute Hepatic Failure (AHF), also called Pediatric Acute Liver Failure (PALF), is a rapidly progressive liver dysfunction occurring in a child without pre-existing chronic liver disease, leading to severe impairment of liver synthetic function and encephalopathy.
It is a medical emergency associated with:
- Massive hepatocellular injury
- Coagulopathy
- Hepatic encephalopathy
- Multi-organ dysfunction
- High mortality without timely management or liver transplantation
According to major pediatric references including AAP, Nelson Textbook of Pediatrics, and ISPGHAN, early recognition and aggressive supportive care are critical for survival.
Definition of Pediatric Acute Liver Failure
Pediatric acute liver failure is defined by:
Essential Criteria
- No evidence of chronic liver disease
- Acute liver injury
- Coagulopathy not corrected by vitamin K
Coagulation Criteria
- INR >1.5 with encephalopathy
OR - INR >2 without encephalopathy
Why Acute Hepatic Failure is Dangerous
The liver performs critical functions:
- Glucose regulation
- Protein synthesis
- Clotting factor production
- Ammonia detoxification
- Drug metabolism
- Immune regulation
When the liver suddenly fails:
- Toxins accumulate
- Cerebral edema develops
- Severe bleeding can occur
- Shock and renal failure may follow
Epidemiology of Pediatric Acute Liver Failure
- Rare but life-threatening condition
- Significant cause of PICU admissions
- Common indication for pediatric liver transplantation
- Mortality remains high despite advances
Common Age Groups
- Infants: metabolic and viral causes
- Older children/adolescents: drugs, autoimmune hepatitis, Wilson disease
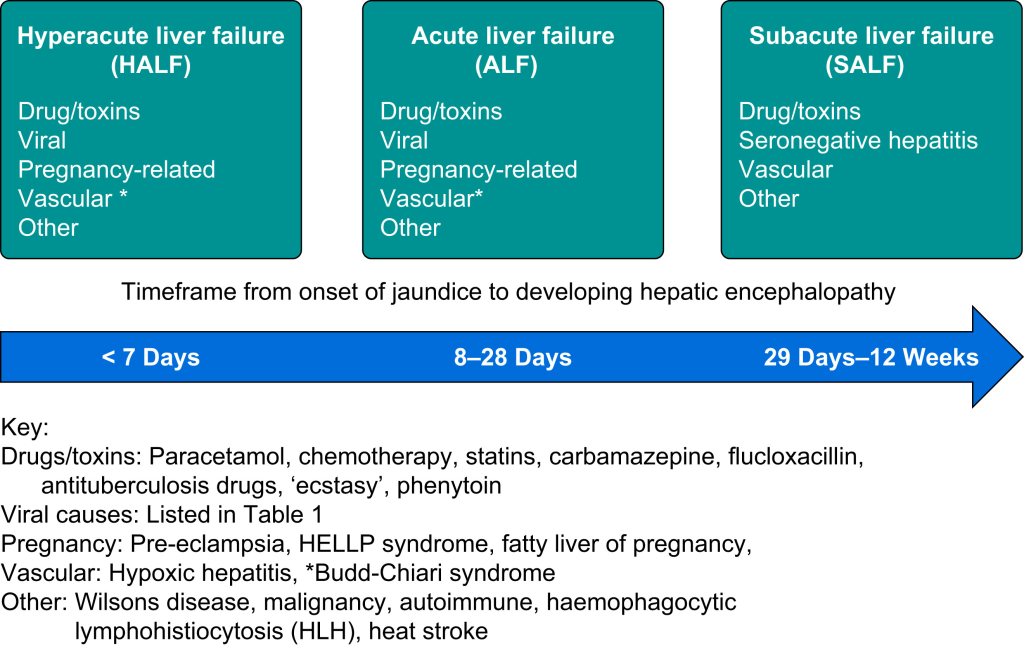
Etiology of Acute Hepatic Failure in Children
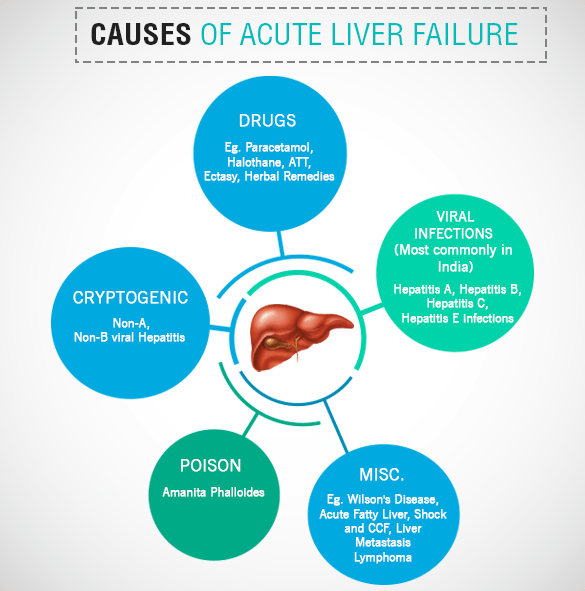
1. Viral Hepatitis
Common Viral Causes
- Hepatitis A
- Hepatitis B
- Hepatitis E
- HSV (especially neonates)
- EBV
- CMV
- Adenovirus
- Enteroviruses
Important Point
In developing countries including Nepal and South Asia:
- Hepatitis A and E remain major causes
2. Drug-Induced Liver Injury (DILI)
Common Drugs
- Acetaminophen (Paracetamol)
- Antitubercular drugs
- Valproate
- Antiepileptics
- Herbal medications
Acetaminophen Toxicity
Most common cause in many developed countries.
Toxic metabolite:
- NAPQI
Normally detoxified by glutathione.
3. Metabolic Disorders
Especially important in infants.
Major Causes
- Galactosemia
- Tyrosinemia
- Mitochondrial disorders
- Fatty acid oxidation defects
- Wilson disease
- Neonatal hemochromatosis
4. Autoimmune Hepatitis
Can present dramatically with:
- Jaundice
- Coagulopathy
- Encephalopathy
Look for:
- ANA
- ASMA
- Elevated IgG
5. Ischemic and Toxic Causes
- Shock liver
- Sepsis
- Mushroom poisoning
- Toxins
6. Indeterminate Causes
A substantial number of pediatric cases remain unexplained despite extensive workup.
Pathophysiology of Acute Hepatic Failure
Hepatocyte Injury
Massive hepatocyte necrosis leads to:
- Failure of detoxification
- Reduced clotting factor synthesis
- Metabolic instability
Hyperammonemia
Ammonia accumulates due to impaired hepatic detoxification.
This causes:
- Astrocyte swelling
- Cerebral edema
- Increased intracranial pressure
Coagulopathy
Liver cannot synthesize:
- Factors II
- V
- VII
- IX
- X
Result:
- Severe bleeding tendency
Immune Dysfunction
Patients become highly susceptible to:
- Sepsis
- Fungal infections
Clinical Features of Acute Hepatic Failure
Early Symptoms
- Nausea
- Vomiting
- Malaise
- Fever
- Abdominal pain
- Poor feeding
- Irritability
Liver-Specific Findings
- Jaundice
- Hepatomegaly
- Tender liver
- Dark urine
- Pale stools
Features of Hepatic Encephalopathy
Stage I
- Irritability
- Sleep disturbances
- Behavioral changes
Stage II
- Confusion
- Drowsiness
- Asterixis
Stage III
- Stupor
- Hyperreflexia
Stage IV
- Coma
Signs of Cerebral Edema
- Hypertension
- Bradycardia
- Unequal pupils
- Abnormal posturing
This is a life-threatening emergency.
Diagnostic Evaluation of Acute Hepatic Failure
Initial Laboratory Workup
Liver Function Tests
- AST/ALT
- Bilirubin
- Albumin
- ALP
- GGT
Synthetic Function
- PT/INR
- Fibrinogen
Metabolic Evaluation
- Blood glucose
- Lactate
- Serum ammonia
- ABG
Viral Studies
- HAV IgM
- HBsAg
- Anti-HBc IgM
- HEV serology
- HSV PCR
Autoimmune Tests
- ANA
- ASMA
- Anti-LKM
- IgG
Metabolic Tests
- Ceruloplasmin
- Urine succinylacetone
- Plasma amino acids
- Urine organic acids
Imaging
Ultrasound Abdomen with Doppler
Useful for:
- Liver size
- Vascular patency
- Ascites
- Chronic liver disease exclusion
Important ICU Monitoring
Continuous monitoring of:
- Mental status
- Blood glucose
- ICP signs
- Urine output
- Electrolytes
- INR
- Ammonia
Management of Acute Hepatic Failure
Core Principles
- PICU admission
- Aggressive supportive care
- Prevent cerebral edema
- Treat underlying cause
- Early transplant referral
Stabilization
Airway
Intubate if:
- Grade III/IV encephalopathy
- Airway compromise
Circulation
Maintain:
- Adequate perfusion
- MAP
- Renal function
Avoid fluid overload.
Management of Hypoglycemia
Frequent glucose monitoring is mandatory.
Treatment:
- Dextrose bolus
- Continuous glucose infusion
Cerebral Edema Management
General Measures
- Head elevation to 30°
- Avoid neck compression
- Minimize stimulation
Osmotherapy
Mannitol
- 0.5–1 g/kg IV
OR
Hypertonic Saline
Target serum sodium:
- 145–150 mEq/L
Ammonia Reduction
Lactulose
Reduces ammonia absorption from gut.
Renal Replacement Therapy
Indicated for:
- Severe hyperammonemia
- Renal failure
Coagulopathy Management
Important principle:
- Do NOT correct INR routinely unless bleeding or procedure planned.
Options
- Vitamin K
- FFP
- Cryoprecipitate
- Platelets
Infection Control
High suspicion for:
- Bacterial infections
- Fungal sepsis
Empiric antibiotics are often used in critically ill patients.
Etiology-Specific Treatment
Acetaminophen Toxicity
N-acetylcysteine (NAC)
Acts by:
- Replenishing glutathione
- Improving hepatic perfusion
N-acetylcysteine restores glutathione and reduces NAPQI toxicity
HSV Hepatitis
- IV acyclovir
Autoimmune Hepatitis
- Corticosteroids
Wilson Disease
Usually requires urgent liver transplantation.
Nutrition in Acute Hepatic Failure
Key Principles
- Early enteral nutrition preferred
- Avoid prolonged fasting
- Adequate calories essential
Protein
Previously restricted heavily, but modern pediatric guidelines recommend:
- Avoid excessive restriction
- Individualize according to encephalopathy severity
Liver Transplantation in Acute Hepatic Failure
Indications
- Progressive encephalopathy
- Refractory coagulopathy
- Severe acidosis
- Persistent hyperammonemia
- Multi-organ failure
Poor Prognostic Factors
- INR worsening
- Severe encephalopathy
- Cerebral edema
- Renal failure
- Rising bilirubin
- Persistent lactic acidosis
Complications of Acute Hepatic Failure
Neurologic
- Cerebral edema
- Seizures
- Herniation
Hematologic
- Bleeding
- DIC
Renal
- Hepatorenal syndrome
- AKI
Infectious
- Sepsis
- Fungal infections
Prognosis
Outcome depends on:
- Etiology
- Speed of recognition
- Availability of transplant
- Degree of encephalopathy
Better Prognosis
- Hepatitis A
- Acetaminophen toxicity (early NAC)
Worse Prognosis
- Wilson disease
- Indeterminate PALF
- Severe cerebral edema
High-Yield Exam Points on Acute Hepatic Failure
Most Important Diagnostic Marker
- Elevated INR
Most Common Cause in Developed Countries
- Acetaminophen toxicity
Major Cause of Death
- Cerebral edema and sepsis
Drug of Choice in Acetaminophen Toxicity
- N-acetylcysteine
Key Emergency
- Raised intracranial pressure
Acute Hepatic Failure Flowchart
Acute Liver Injury
↓
Coagulopathy (INR ↑)
↓
Evaluate Etiology
↓
PICU Supportive Care
↓
Prevent Cerebral Edema
↓
Treat Specific Cause
↓
Assess for Liver TransplantFrequently Asked Questions (FAQs)
Is acute hepatic failure reversible?
Yes. Some causes recover completely with early management, while others require liver transplantation.
What is the most dangerous complication?
Cerebral edema leading to brain herniation.
Why is ammonia elevated?
The failing liver cannot convert ammonia into urea effectively.
Can children survive without liver transplant?
Yes, depending on etiology and severity. Hepatitis A-related PALF often recovers spontaneously.
Key Takeaway
Acute hepatic failure in children is a rapidly progressive and potentially fatal condition requiring:
- Early diagnosis
- Intensive monitoring
- Prevention of cerebral edema
- Etiology-directed therapy
- Timely liver transplantation evaluation
Rapid recognition and evidence-based critical care significantly improve survival outcomes.





