Table of Contents
Polycystic Ovary Syndrome (PCOS / PCOD) — High-Yield Notes
Based on international evidence-based guidelines, Endocrine Society, ACOG, and peer-reviewed literature. (NCBI)
Definition
- PCOS = common endocrine-metabolic disorder in reproductive-age women
- Characterized by:
- Hyperandrogenism
- Ovulatory dysfunction
- Polycystic ovarian morphology
- Associated with:
- Insulin resistance
- Obesity
- Infertility
- Metabolic syndrome
Etiopathogenesis
Multifactorial Disorder
- Genetic predisposition
- Environmental factors
- Hormonal dysregulation
- Insulin resistance
Core Pathophysiology
1. Increased LH secretion
- ↑ GnRH pulse frequency → preferential LH secretion
- ↑ LH stimulates theca cells
- ↑ androgen production
2. Insulin resistance
- Present in many patients (even lean PCOS)
- Hyperinsulinemia:
- Stimulates ovarian androgen synthesis
- Suppresses SHBG production in liver
- ↑ free testosterone
3. Follicular arrest
- Failure of dominant follicle maturation
- Multiple immature follicles accumulate
4. Hyperandrogenism
- Causes:
- Hirsutism
- Acne
- Alopecia
- Menstrual irregularity
Diagnostic Criteria (Rotterdam Criteria)
Diagnosis requires 2 out of 3 after excluding other causes: (NCBI)
A. Ovulatory Dysfunction
- Oligomenorrhea
- Amenorrhea
- Anovulation
Menstrual abnormalities
- Cycle >35 days
- <8 cycles/year
B. Hyperandrogenism
Clinical
- Hirsutism
- Acne
- Androgenic alopecia
Biochemical
- ↑ Total testosterone
- ↑ Free testosterone
- ↑ DHEAS
C. Polycystic Ovarian Morphology (USG)
- ≥20 follicles per ovary OR
- Ovarian volume >10 mL
Classic appearance
- “String of pearls”
Important Diagnostic Point
- PCOS is a diagnosis of exclusion. (OUP Academic)
Differential Diagnoses to Exclude
Endocrine causes
- Hypothyroidism
- Hyperprolactinemia
- Cushing syndrome
- Congenital adrenal hyperplasia
- Androgen-secreting tumors
Others
- Acromegaly
- Premature ovarian insufficiency
Clinical Features
Menstrual
- Oligomenorrhea
- Amenorrhea
- Irregular cycles
- Infertility
Hyperandrogenic Features
- Hirsutism
- Acne
- Alopecia
- Seborrhea
Metabolic Features
- Obesity
- Central obesity
- Insulin resistance
- Acanthosis nigricans
Reproductive Features
- Subfertility/infertility
- Recurrent miscarriage
Psychological Associations
- Anxiety
- Depression
- Eating disorders
- Poor body image
Investigations
Hormonal Tests
- Total/free testosterone
- DHEAS
- LH, FSH
- Prolactin
- TSH
- 17-hydroxyprogesterone
Metabolic Screening
- Fasting glucose
- HbA1c
- Lipid profile
- OGTT (high-risk patients)
Imaging
- Pelvic ultrasonography
Typical Laboratory Findings
- ↑ LH:FSH ratio (>2:1 sometimes)
- ↑ Testosterone
- ↑ Insulin
- ↓ SHBG
Complications
Reproductive
- Infertility
- Anovulation
- Pregnancy complications
Metabolic
- Type 2 diabetes mellitus
- Dyslipidemia
- Metabolic syndrome
- Hypertension
Cardiovascular
- Increased long-term CV risk
Endometrial
- Endometrial hyperplasia
- Endometrial carcinoma
- Due to chronic unopposed estrogen
Management
1. Lifestyle Modification (First-line)
- Weight reduction
- Exercise
- Calorie restriction
- Low glycemic diet
Benefits
- Improves ovulation
- Reduces insulin resistance
- Improves fertility
2. Menstrual Irregularity Management
Combined Oral Contraceptive Pills (COCPs)
- First-line for nonfertility symptoms
- Benefits:
- Regular cycles
- ↓ androgen production
- Improves acne/hirsutism
3. Hirsutism & Acne
Antiandrogens
- Spironolactone
- Finasteride
- Flutamide (rare due to hepatotoxicity)
Important
- Use contraception with antiandrogens
4. Insulin Resistance
Metformin
- Improves insulin sensitivity
- May restore ovulation
- Useful in:
- Obesity
- Prediabetes
- Metabolic syndrome
5. Infertility Treatment
First-line Ovulation Induction
- Letrozole (preferred)
- Clomiphene citrate
Others
- Gonadotropins
- IVF if resistant
Pregnancy Risks in PCOS
- Gestational diabetes
- Pregnancy-induced hypertension
- Preeclampsia
- Preterm birth
Adolescent PCOS
- Diagnosis difficult soon after menarche
- Physiologic irregular cycles common
- Ultrasound less reliable in adolescents (NCBI)
High-Yield Exam Pearls
- Most accepted criteria = Rotterdam criteria
- Need 2 out of 3 criteria
- PCOS is a diagnosis of exclusion
- Most common cause of anovulatory infertility
- Insulin resistance is central mechanism
- Chronic anovulation → unopposed estrogen → endometrial cancer risk
- First-line treatment = lifestyle modification
- First-line ovulation induction = letrozole
- COCPs are first-line for menstrual symptoms
- “String of pearls” appearance on USG
Very Short Summary
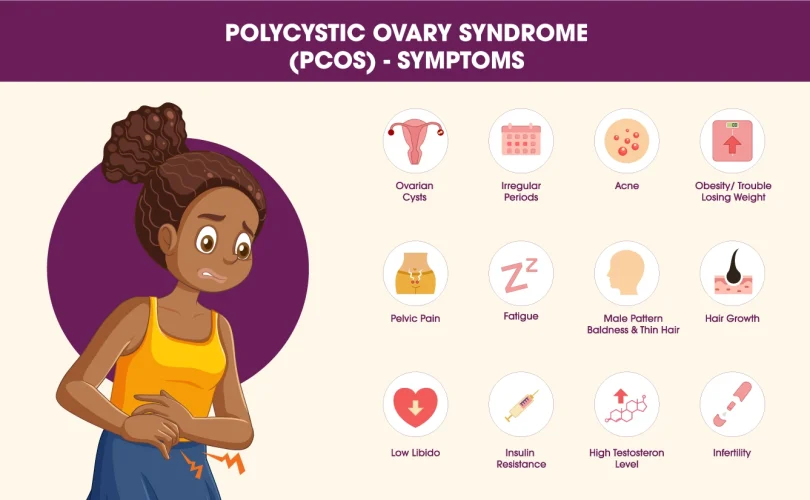
PCOS is a common endocrine disorder characterized by:
- Hyperandrogenism
- Irregular ovulation
- Polycystic ovaries
Main problems:
- Irregular periods
- Infertility
- Hirsutism
- Obesity
- Insulin resistance
Treatment:
- Lifestyle change
- COCPs
- Metformin
- Letrozole for fertility
Renaming PCOS to PMOS
Yes — there has been a major recent international change in terminology.
New Name for PCOS
The condition previously called PCOS (Polycystic Ovary Syndrome) has officially been renamed:
PMOS
Polyendocrine Metabolic Ovarian Syndrome
This was announced in 2026 after a 14-year international consensus effort involving:
- Endocrinologists
- Gynecologists
- Researchers
- Patient advocacy groups
- More than 50 global medical organizations (The Guardian)
Why Was the Name Changed?
Experts felt the term “PCOS” was misleading because:
- Many patients do not actually have ovarian cysts
- The disorder affects multiple body systems, not only ovaries
- The old name caused:
- Delayed diagnosis
- Confusion
- Stigma
- Under-recognition of metabolic disease
The new term “PMOS” better reflects:
- Endocrine dysfunction
- Metabolic abnormalities
- Hormonal imbalance
- Reproductive effects (The Guardian)
Full Form Breakdown
P — Polyendocrine
Multiple hormone systems are involved
M — Metabolic
Strong association with:
- Insulin resistance
- Obesity
- Diabetes
- Dyslipidemia
O — Ovarian
Ovarian dysfunction and ovulatory problems remain important
S — Syndrome
Collection of related clinical features
Important Clinical Point
Diagnostic criteria remain essentially the same.
The name changed, but the underlying disorder and diagnostic approach remain based on established international criteria. (The Cut)
Key Facts
- Affects approximately 1 in 8 women worldwide
- Estimated >170 million affected globally
- Strongly associated with:
- Infertility
- Metabolic syndrome
- Type 2 diabetes
- Cardiovascular risk
- Mental health disorders (endocrine.org)
Transition Timeline
International organizations plan gradual adoption of the term PMOS in:
- Clinical guidelines
- Research papers
- Medical education
- Public awareness campaigns
Implementation is expected over the next few years. (The Guardian)