Pediatric Nutrition — Practice MCQs Free For You All
Section 1: Questions Q1. According to WHO/AAP recommendations, exclusive breastfeeding …
Pediatrics and Neonatology and adolescent medicine
Pediatrics and Neonatology and adolescent medicine
Browsing Year
Section 1: Questions Q1. According to WHO/AAP recommendations, exclusive breastfeeding …
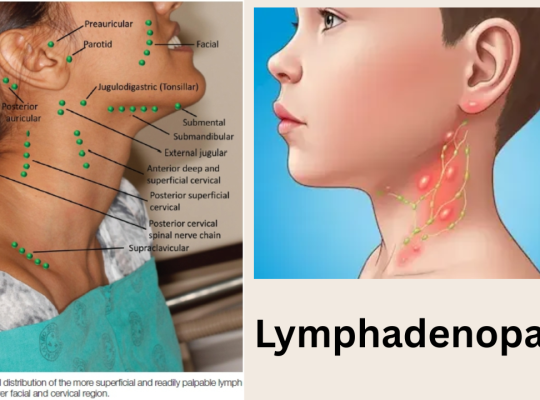
Introduction The definition of significant lymph node enlargement depends on …
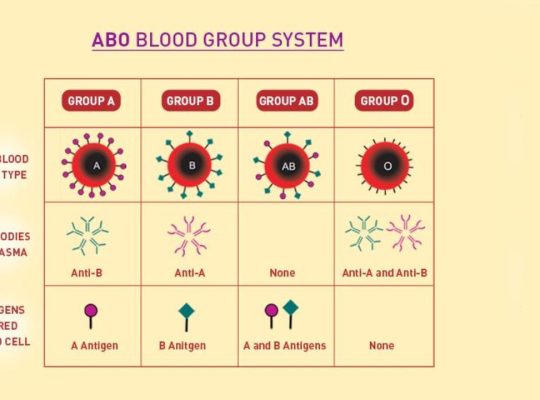
MAL Blood Group · Published in Blood Journal · 2024 …
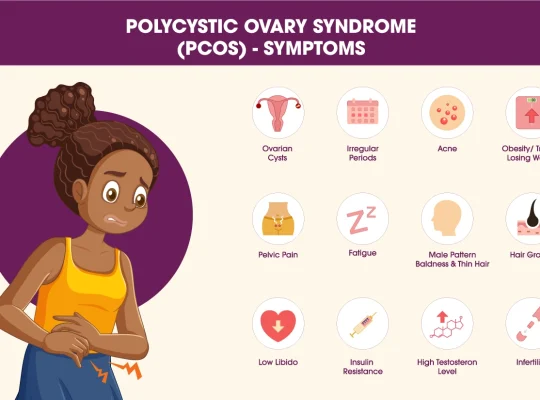
Polycystic Ovary Syndrome (PCOS / PCOD) — High-Yield Notes Based …
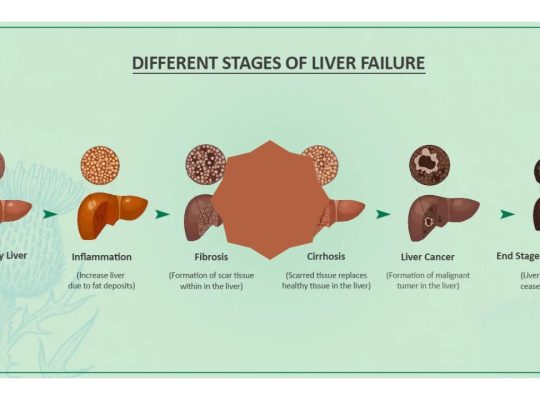
What is Acute Hepatic Failure? Acute Hepatic Failure (AHF), also …

Introduction Neonatal resuscitation is one of the most time-sensitive and …
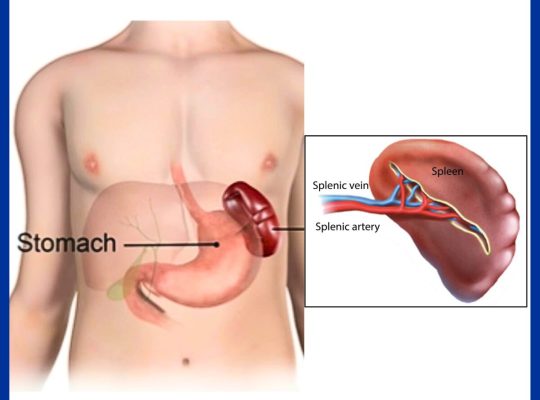
Introduction While most people can easily point to their heart …
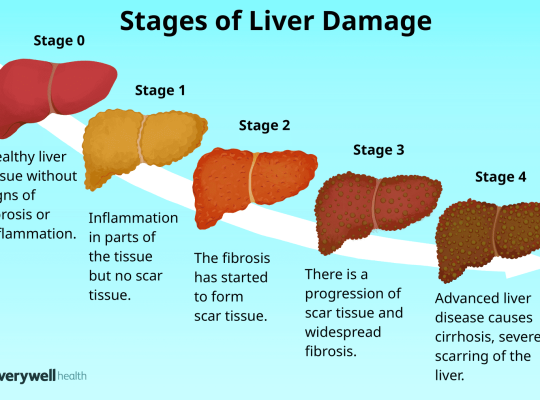
📘 Standard Pediatric Definition (Nelson Textbook of Pediatrics) 👉 Acute …
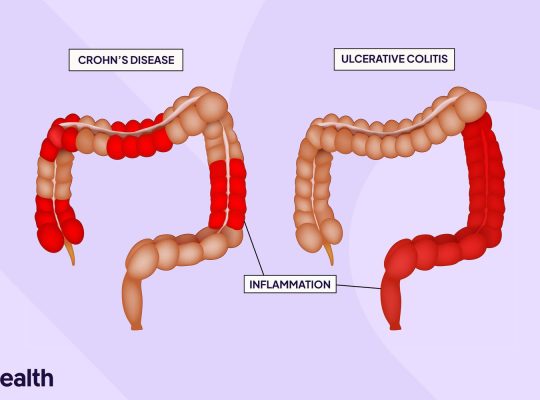
Video on Chron’s Disease (sensitizer) 🔬 Overview & Definition Crohn’s …

लोक सेवा आयोग नेपाल स्वास्थ्य सेवा, जनरल नर्सिङ समूह, सातौं …